Assessment of mitral stenosis by echocardiography
Assessment of mitral stenosis by echocardiography
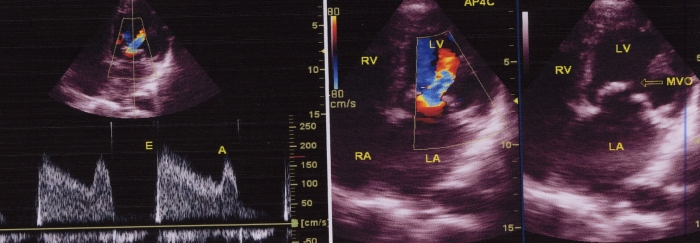
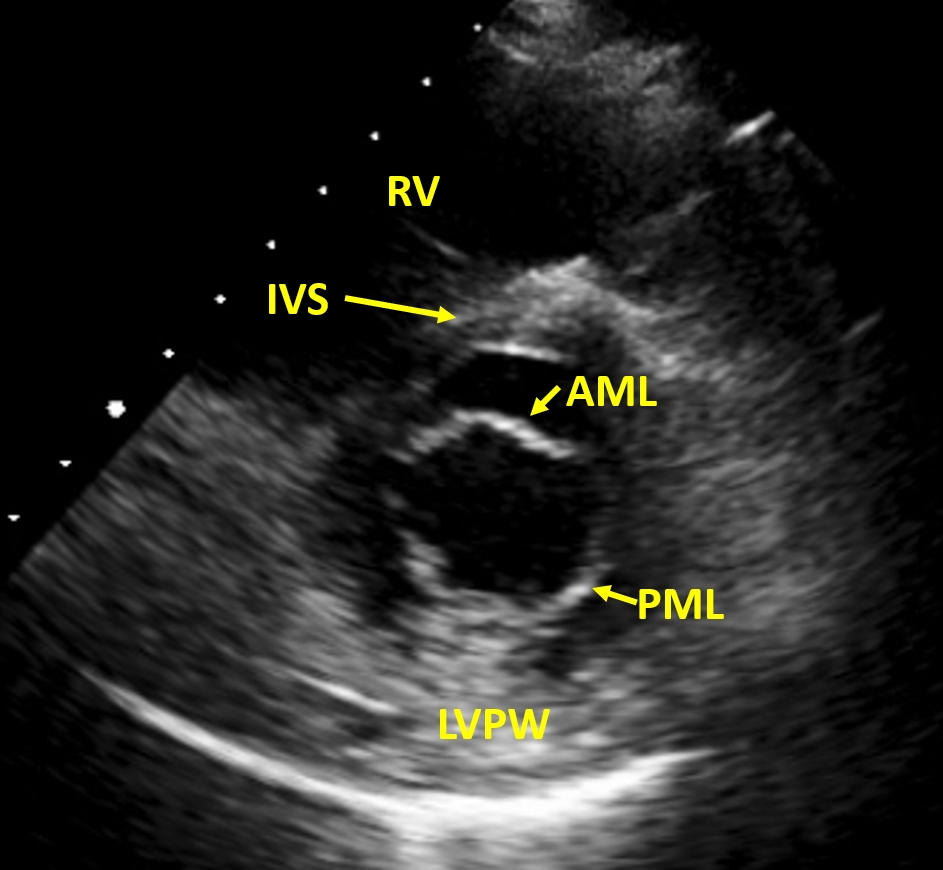
Right panel shows the parasternal long axis view. Doming of the anterior mitral leaflet is seen well and has the appearance of hockey stick. This appearance is classical of rheumatic mitral stenosis. Paradoxical movement of the posterior mitral leaflet is also visible. Normally posterior mitral leaflet moves posteriorly in diastole. Here there is a paradoxical anterior movement due to commissural fusion. Left atrium is dilated. Left panel shows parasternal short axis view. The mitral orifice is seen within the cross section of the left ventricle. The anterior and posterior leaflets are seen in cross section and are thickened; the commissures are fused. Parasternal long axis view will give an assessment of the subvalvar apparatus. Subvalvar fusion may result in poor results after valvotomy as they can produce secondary obstruction beyond the valve. Parasternal short axis view is used for quantitating the severity of mitral stenosis by using planimetry to measure the mitral valve orifice. Commissural fusion and calcification if present can be seen well on PSAX view. Trans mitral gradient is better assessed in apical four chamber view by Doppler. Associated tricuspid regurgitation if present, can be seen on apical four chamber view, which will also help in estimating the right ventricular systolic pressure from the TR.

Parasternal short axis view in mitral stenosis, showing the “fish mouth appearance” of the mitral orifice in cross section.
Normal mitral valve cross section for comparison showing anterior and posterior mitral leaflets widely separated. Scallops of mitral leaflets are also visible, more clearly in the posterior leaflet. Read Carpentier nomenclature of mitral leaflet scallops. The leaflets of normal mitral valve are thin, pliable, non calcified and open well in diastole, with valve area of 4-6 square centimeters. Opening of a normal mitral valve may be reduced in low cardiac output states, even without significant mitral stenosis.
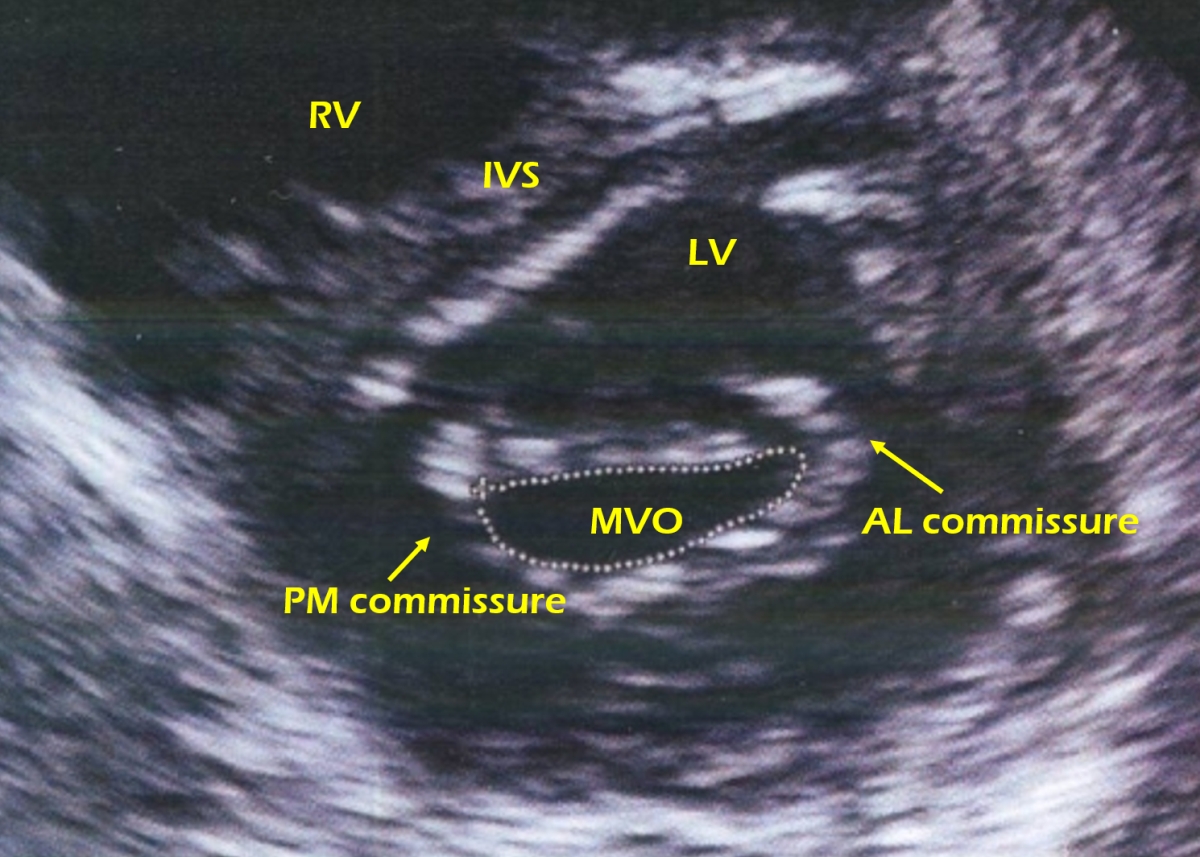
Parasternal short axis view showing mitral valve in cross section and anterolateral and posteromedial commissures. The valve leaflets are thickened and the commissures are fused. The cut is slightly oblique as a good cut should appear circular. It is often difficult to get a good circular outline of the mitral valve due to varying anatomical features of the chambers and cardiac position. Ideally the smallest full circle should be taken to planimeter the valve area. If it is not a full circle, the subvalvar pathology may be measured as the valve orifice. If the smallest full circle is not taken, it will be the valve proximal to the severest stenosis (valve belly).
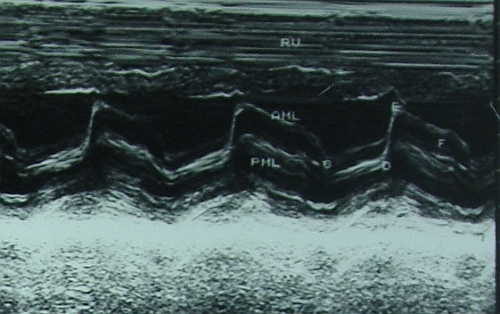
M mode echocardiogram showing the paradoxical anterior motion of posterior mitral leaflet in diastole with reduced separation of the two leaflets. Anterior mitral leaflet has certain points marked in its movement: C, D,E and F. The EF slope is reduced in mitral stenosis – it becomes almost flat in severe mitral stenosis. CD is the closed position of the mitral leaflets in systole and DE is the opening excursion of the anterior mitral leaflet. A wave on M-Mode echocardiogram is absent in mitral stenosis.
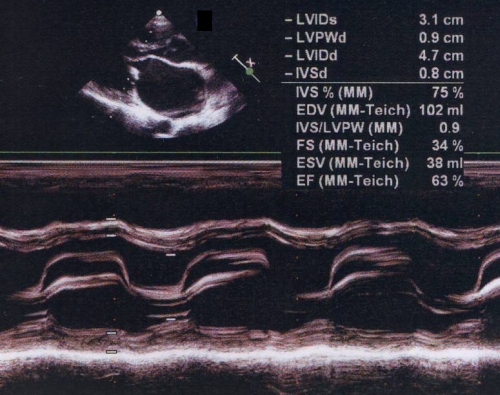
M-mode echocardiogram in mitral stenosis showing the flat EF slope and paradoxical motion of posterior mitral leaflet. Normally the anterior mitral leaflet shows an M shaped anterior movement and posterior mitral leaflet shows a smaller W shaped posterior movement pattern. The upper panel shows the doming of anterior mitral leaflet in diastole.
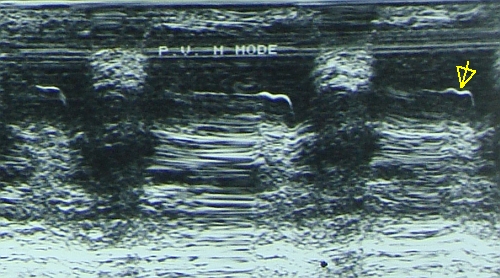
Mitral stenosis with pulmonary hypertension as evidenced by the flat EF slope of the pulmonary valve M mode echocardiogram and the shallow a wave, marked by the arrow. A mid systolic notch may also appear in severe pulmonary hypertension. When Doppler echo was not available, M mode of the pulmonary valve was an important tool to assess pulmonary hypertension.
Assessment of Mitral Valve Area by Echo – 3D Planimetry, PHT, PISA
Wilkins Echocardiographic Score for Mitral Stenosis
Low Gradient Severe Mitral Stenosis
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal