Chest X-ray in left to right shunts
Chest X-ray in left to right shunts
Chest X-ray is a simple, cheap and easily available investigation for the evaluation of left to right shunts. But it is often avoided in pediatric age group due to concerns of radiation. Cardiac size and lung vascularity can be readily assessed and followed up serially [1]. Lung vascularity pattern is different in pre-tricuspid and post tricuspid shunts. Pattern changes with the development of pulmonary hypertension as the shunt decreases. Cardiac size also decreases when the shunt decreases. Cardiac chamber enlargements are also different according to the level of shunt.
Chest X-ray in atrial septal defect
Atrial septal defect (ASD) is the most common congenital heart disease in the adult. It is a pre-tricuspid shunt.
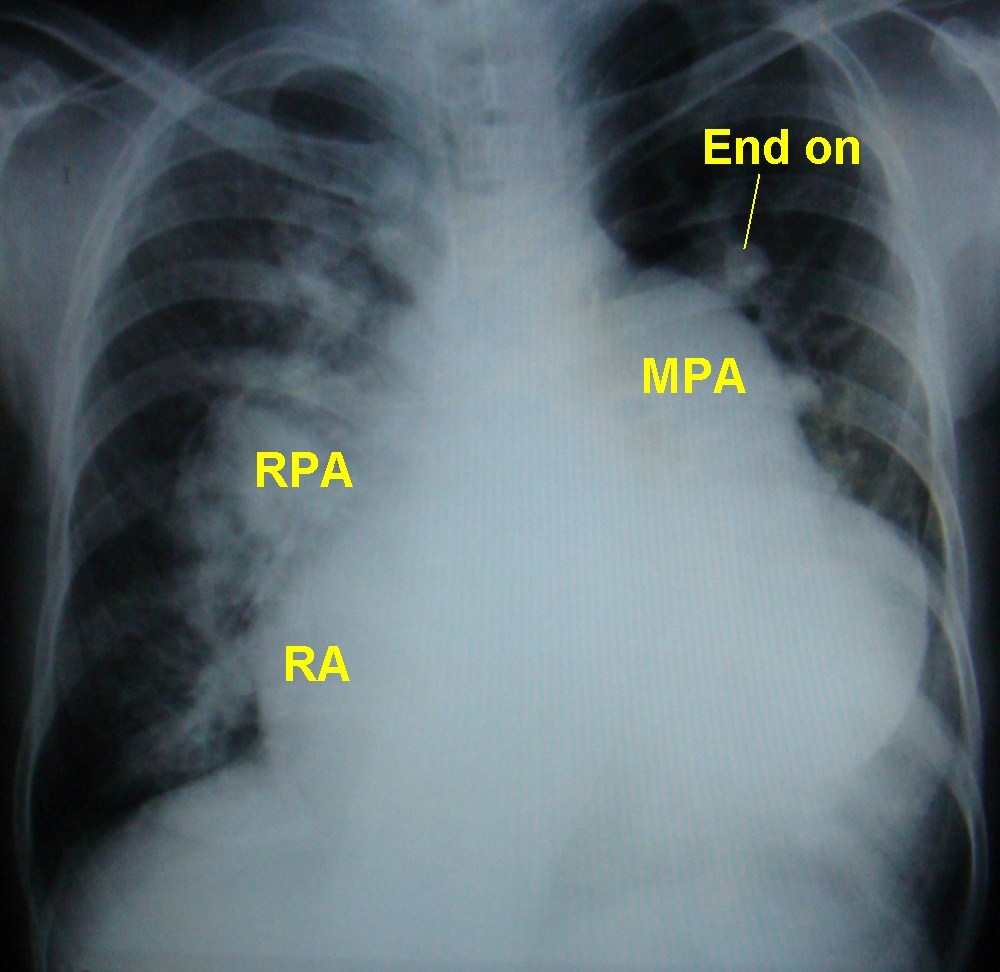
This chest X-ray in ASD shows grossly dilated main pulmonary artery. The right pulmonary artery is also quite enlarged. Right atrial enlargement is seen as a shift of the cardiac contour to the right of the spine. Pulmonary vascularity is increased and prominent end on vessels are also seen. Apex is upwards, suggesting a right ventricular configuration. All features suggest a large secundum atrial septal defect with a large left to right shunt producing severe pulmonary hypertension. Cardiomegaly on chest x-ray is suggestive of atrial septal defect in Eisenmenger syndrome, while it is unlikely in ventricular septal defect and patent ductus arteriosus. Cardiomegaly is mainly due to the grossly dilated right atrium in atrial septal defect. The right atrium is not enlarged in the other two varieties of Eisenmenger syndrome. In ventricular septal defect with large left to right shunt, the cardiac size comes down as pulmonary hypertension develops and the shunt decreases. Cardiomegaly in ventricular septal defect and patent ductus arteriosus with large left to right shunt are due to left ventricular enlargement. But this comes down with the development of pulmonary hypertension. That is why cardiomegaly is not a feature of Eisenmenger syndrome due to ventricular septal defect and patent ductus arteriosus.

Prominent main pulmonary artery, right pulmonary artery and left pulmonary artery (behind the main pulmonary artery) and end on views of dilated branch pulmonary arteries are seen. Echocardiography documented large secundum ASD with severe pulmonary hypertension and bidirectional shunt across the ASD. There is mild right atrial enlargement and the configuration of the apex is right ventricular.
Fleischner’s sign
Prominent central pulmonary artery in acute massive pulmonary embolism is called Fleischner’s sign [2]. Some authors extend the term to prominent central pulmonary artery due to other causes of pulmonary hypertension as in atrial septal defect [3].
X-ray chest in ventricular septal defect
Chest X-ray is normal in a small ventricular septal defect. Large ventricular septal defect will have left ventricular type of cardiomegaly and pulmonary congestion in infancy before the development of pulmonary hypertension. Pulmonary hypertension manifests on CXR as prominent main pulmonary artery segment and prominent right descending pulmonary artery. Close scrutiny may show the dilated left pulmonary artery within the cardiac silhouette. When severe pulmonary hypertension occurs, cardiac size decreases due to decrease in the pulmonary blood flow. But pulmonary arteries become more prominent. Initially pulmonary vascular markings are prominent and seen up to the periphery of the lung fields with large left to right shunt. When vasoreactive pulmonary hypertension sets in there is peripheral pruning with decrease in vascular markings in the periphery of the lung fields.
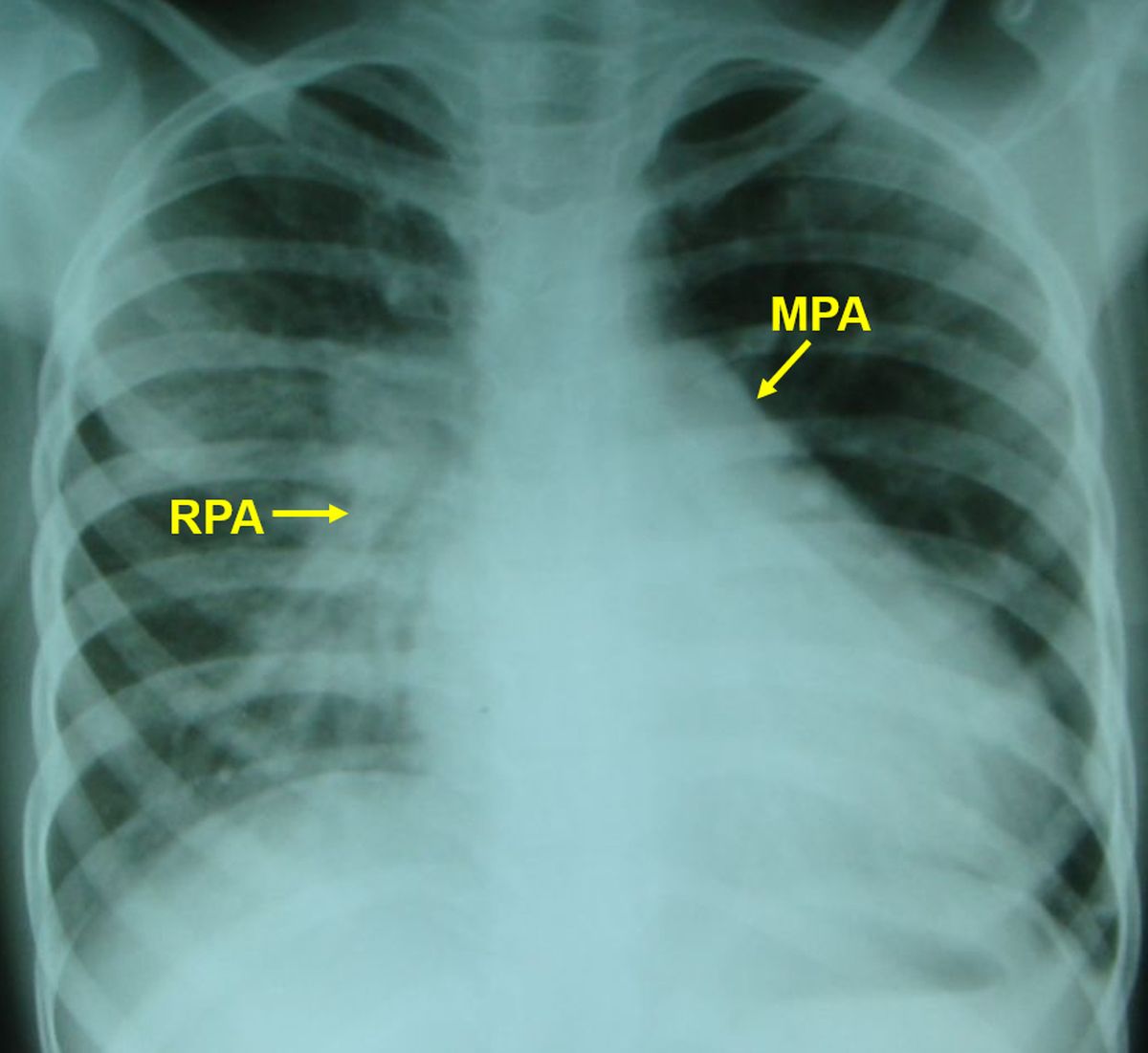
X-Ray chest PA View of a child with ventricular septal defect and left to right shunt and hyperdynamic pulmonary hypertension. There is cardiomegaly, prominent main pulmonary artery segment and right pulmonary artery. Enlarged left pulmonary artery shadow is seen below the left cardiac border, within the cardiac silhouette. The enhanced vascular markings are visible on the right side whereas it is obscured by the cardiac shadow on the left side. This child ideally needs cardiac catheterization for evaluation of shunt and pulmonary vascular resistance and its reversibility to decide on surgical option.
X-ray chest in patent ductus arteriosus
X-ray chest in patent ductus arteriosus with large left to right shunt will show cardiomegaly and increased pulmonary vascularity as in other large left to right shunts. In patent ductus arteriosus, an additional feature on x-ray chest is the dilated aortic shadow. Inverted Y shaped ductal calcification may also be seen with patent ductus arteriosus and Eisenmenger syndrome.
X-ray chest in partial anomalous pulmonary venous drainage
Usually partial anomalous pulmonary venous drainage is associated with sinus venosus atrial septal defect and the X-ray findings are those of atrial septal defect. In isolated partial anomalous pulmonary venous drainage, one specific variety is Scimitar syndrome. Scimitar syndrome is characterized by partial anomalous pulmonary venous drainage of right lung, right lung hypoplasia, dextroposition of heart, and anomalous systemic arterial supply from aorta or one of its branches to the right lung (sequestration) [4]. In Scimitar syndrome partial anomalous pulmonary venous drainage from the right lung is into the inferior vena cava [5]. In partial anomalous pulmonary venous drainage associated with ASD, it usually drains to the superior vena cava right atrium junction.
The partial anomalous pulmonary venous drainage in Scimitar syndrome appears as a curved shadow in the right lower zone, resembling a curved sword which was known as scimitar. The shadow dips down below the diaphragm as it courses towards the inferior vena cava. Familial scimitar syndrome has been reported in two sisters [5].
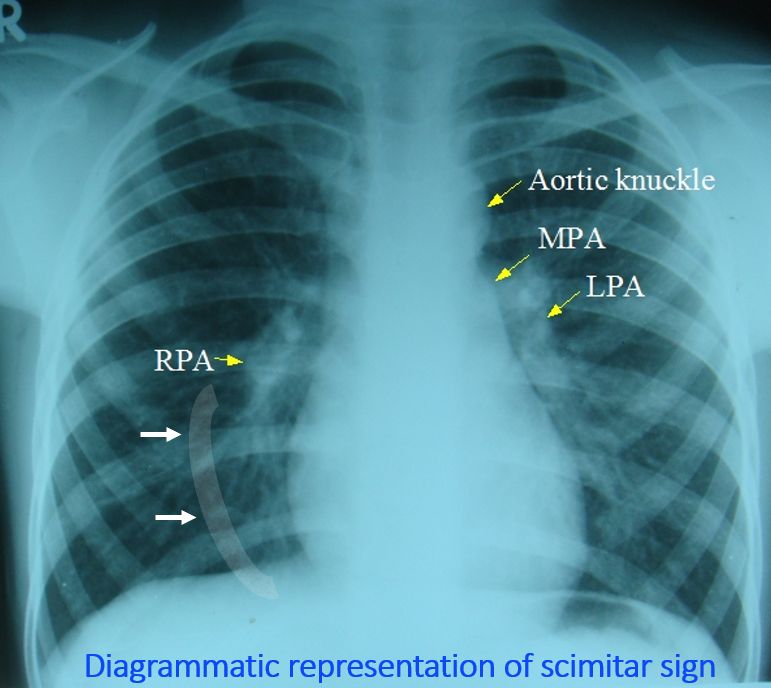
Diagram of a partial anomalous pulmonary vein draining towards the inferior vena cava from the right lung has been superimposed on a chest X-ray and marked by white arrows.
References
- Somerville J, Grech V. The chest x-ray in congenital heart disease 1. Total anomalous pulmonary venous drainage and coarctation of the aorta. Images Paediatr Cardiol. 2009 Jan;11(1):7-9.
- Cooksley T, Husein B, Iqbal J, Bright J. Fleischner’s sign in a massive pulmonary embolism. J Emerg Med. 2012 Jun;42(6):698-9.
- Rigatelli G, Zuin M. Diagnostic chest X-ray in atrial septal defects. J Geriatr Cardiol. 2020 Feb;17(2):125.
- Gupta ML, Bagarhatta R, Sinha J. Scimitar syndrome: A rare disease with unusual presentation. Lung India. 2009 Jan;26(1):26-9.
- Mordue BC. A case series of five infants with scimitar syndrome. Adv Neonatal Care. 2003 Jun;3(3):121-32.
- Ashida K, Itoh A, Naruko T, Otsuka M, Sakanoue Y, Kobayashi M, Yamashita H, Nagashima M, Shinsato T, Takanashi S, Shimizu Y, Haze K. Familial scimitar syndrome: three-dimensional visualization of anomalous pulmonary vein in young sisters. Circulation. 2001 Jun 26;103(25):E126-7.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal