Assessment of right ventricular diastolic function
Assessment of right ventricular diastolic function
Assessment of right ventricular diastolic function is often done by echocardiography, though not as commonly as for the left ventricle. An RV focussed apical four chamber view is used for the assessment of right ventricle. In RV focussed view, transducer is adjusted from the standard apical four chamber view to have right ventricle in the centre of the image than the usual image centered on the left ventricle. The left ventricular outflow tract should not come into the view and left ventricular apex should remain at the top of the image sector. In this adjusted view, the entire right ventricular free wall should be visible [1].
Right ventricular diastolic dysfunction may be associated with various congenital heart diseases, cardiomyopathies, left sided valvular heart disease and systemic conditions like diabetes mellitus, rheumatoid arthritis and conditions causing vasculitis. Assessment of right atrium, right ventricle and inferior vena cava by two-dimensional echocardiography gives indirect evidence on right ventricular diastolic function. This is so because significant elevation of right sided filling pressures would alter the right heart dimensions, size of the inferior vena cava and its inspiratory collapse.
As in the case of mitral valve, assessment of tricuspid inflow velocities is a simple way to assess right ventricular diastolic function. E/A ratio and deceleration time of the E wave can be recorded using pulsed Doppler cursor at the tip of tricuspid valve leaflets. It may be noted that tricuspid flow is highly sensitive to preload, afterload and phase of respiration. Hence averaging 5 consecutive beats or measurement in held expiration have been recommended. As on the left side, absence of A wave in atrial fibrillation would mean that E/A ratio cannot be measured.
Tissue Doppler at lateral tricuspid annulus can be used to measure the E’, A’ and E’/A’ ratio. Right ventricular isovolumic relaxation time (IVRT) can be calculated using tissue Doppler. E/E’ ratio can also be calculated as on the left side. Similarly, Tei index or myocardial performance index can also be calculated. Right ventricular tissue Doppler indices are less load dependent than pulsed Doppler right ventricular inflow measurements.
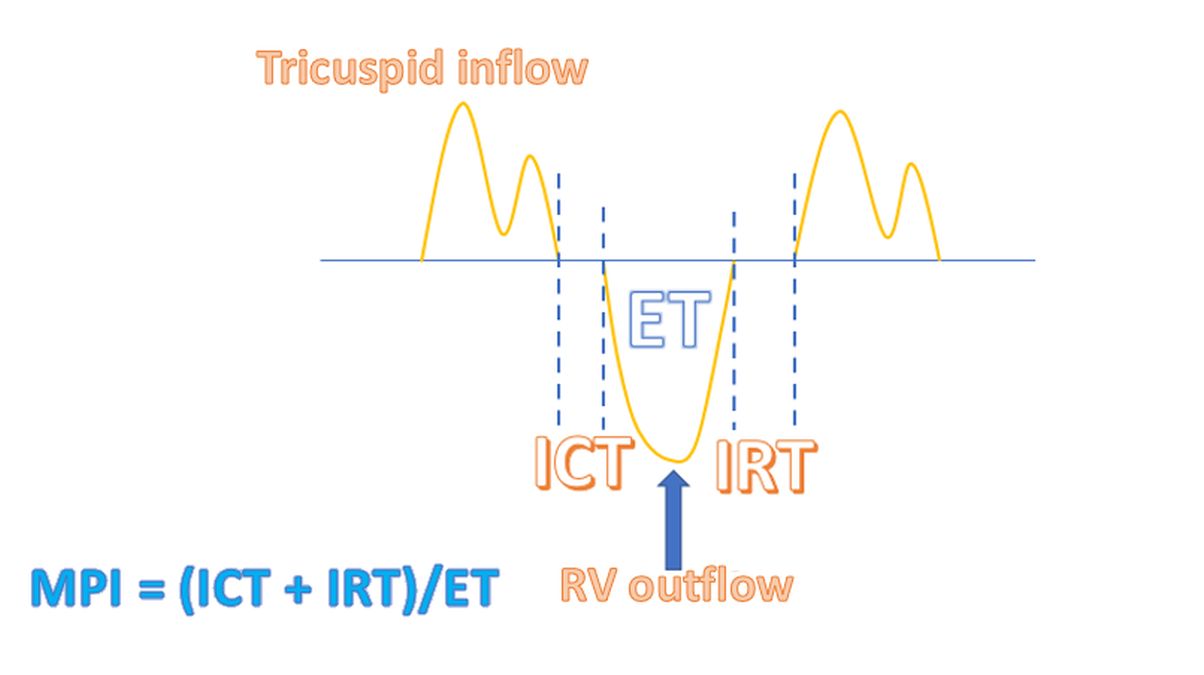
Myocardial performance index (MPI) is the ratio of the time spent in isovolumetric activity divided by the time spent in ventricular ejection [2].
MPI = (ICT + IRT) / ET
ICT: isovolumic contraction time; IRT: isovolumic relaxation time; ET: ejection time
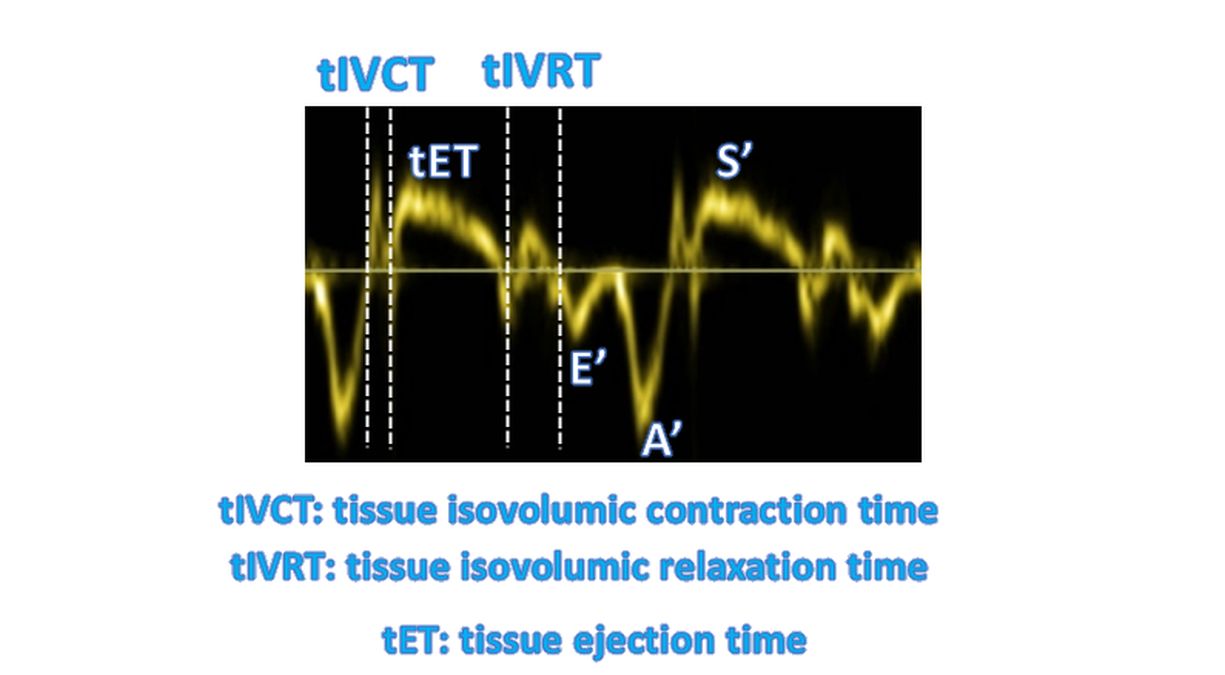
Tei index can also be measured indirectly from the tissue Doppler. It is designated as tMPI [3]. Corresponding measurements on tissue Doppler are tIVCT: tissue isovolumic contraction time, tIVRT: tissue isovolumic relaxation time and tET: tissue ejection time. Measurements are taken using pulsed tissue Doppler from the lateral tricuspid annulus.
Pulsed wave Doppler interrogation of hepatic vein flow is another method of assessing right ventricular diastolic function. Interrogation is done from the subcostal view. As in case of other right sided parameters, velocities are more in inspiration. Hence averaging of 5 consecutive beats is recommended. Hepatic vein Doppler shows systolic S wave, systolic reversal SR wave, diastolic D wave and atrial reversal AR wave. Normally S wave is dominant as IVC fills rapidly and empties the right atrium in ventricular systole. Small SR wave may be seen in late systole. D velocity occurs during right atrial emptying in diastole. A small AR wave is seen in late diastole when atrial contraction completes right ventricular filling along with small backflow into the hepatic veins.
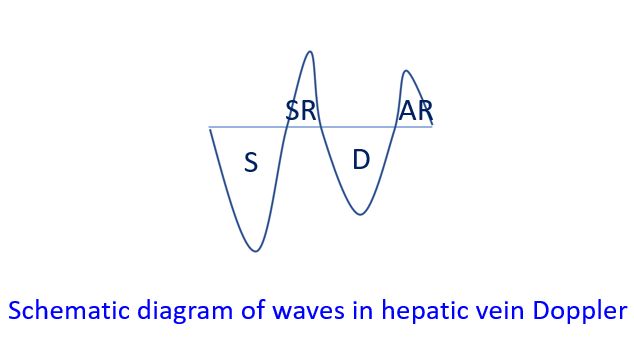
In right ventricular diastolic dysfunction, there is diastolic flow predominance with S/D reversal. Other reversal velocities are also increased in right ventricular diastolic dysfunction, more so in inspiration [1].
References
- Zaidi A, Knight DS, Augustine DX, Harkness A, Oxborough D, Pearce K, Ring L, Robinson S, Stout M, Willis J, Sharma V; Education Committee of the British Society of Echocardiography. Echocardiographic assessment of the right heart in adults: a practical guideline from the British Society of Echocardiography. Echo Res Pract. 2020 Feb 27;7(1):G19-G41. doi: 10.1530/ERP-19-0051. PMID: 32105053; PMCID: PMC7077526.
- Bleeker GB, Steendijk P, Holman ER, Yu CM, Breithardt OA, Kaandorp TA, Schalij MJ, van der Wall EE, Nihoyannopoulos P, Bax JJ. Assessing right ventricular function: the role of echocardiography and complementary technologies. Heart. 2006 Apr;92 Suppl 1:i19-26.
- Zimbarra Cabrita I, Ruisanchez C, Dawson D, Grapsa J, North B, Howard LS, Pinto FJ, Nihoyannopoulos P, Gibbs JS. Right ventricular function in patients with pulmonary hypertension; the value of myocardial performance index measured by tissue Doppler imaging. Eur J Echocardiogr. 2010 Sep;11(8):719-24. doi: 10.1093/ejechocard/jeq051. Epub 2010 Apr 21. PMID: 20410189.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal