Right ventricular function by echocardiography
Right ventricular function by echocardiography
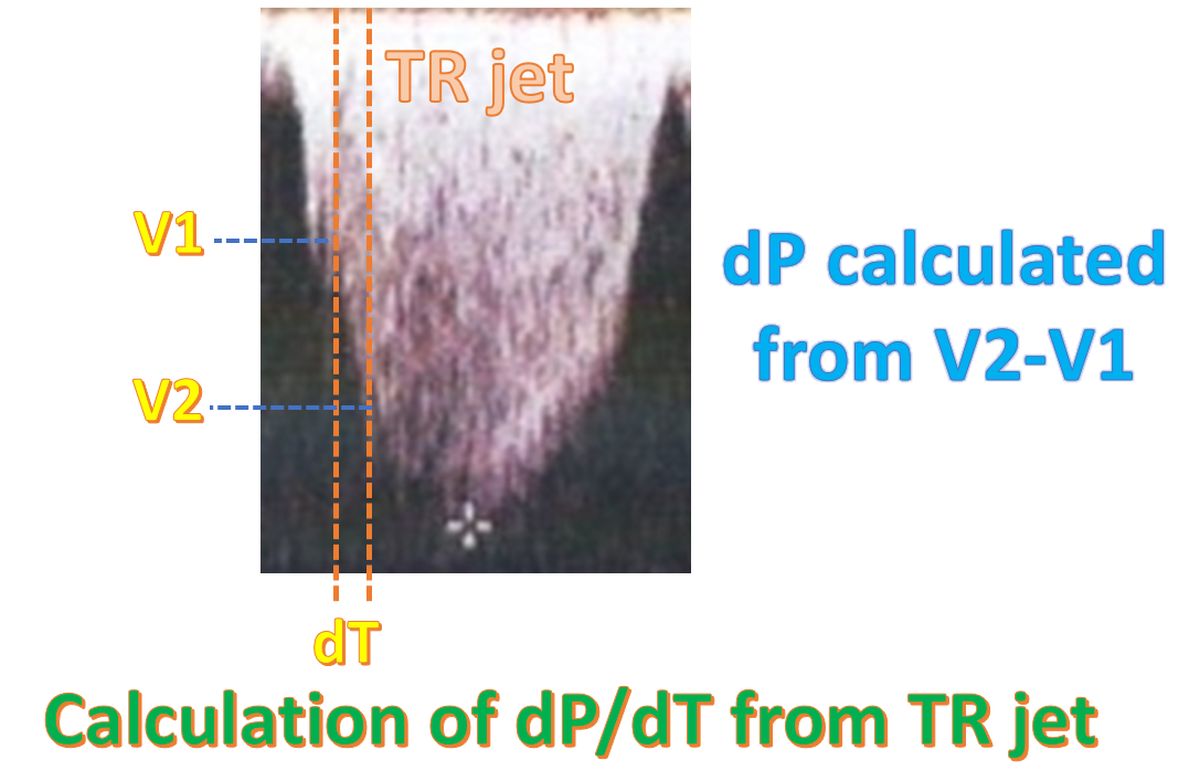
Right ventricular systolic function can be evaluated in terms of right ventricular fractional area change and right ventricular ejection fraction. There are other Doppler and strain imaging methods as well. Right ventricular dP/dt or rate of rise of right ventricular pressure can be estimated from the tricuspid regurgitation Doppler jet. While the left ventricular dP/dt is over 1200 mm Hg/second, that of the right ventricle is over 400 mm Hg/ second [1].
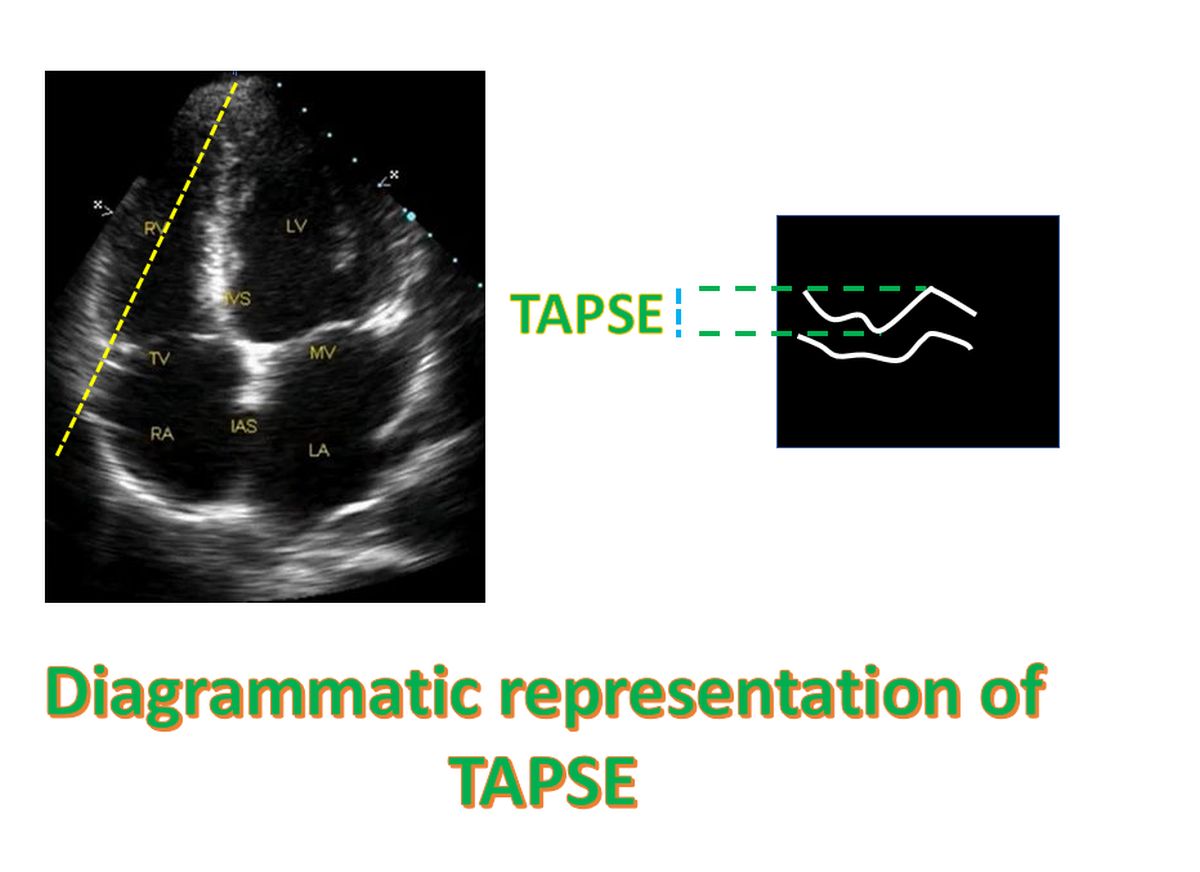
Tricuspid annular plane systolic excursion (TAPSE) is another measure of right ventricular systolic function. It can be measured in the four chamber view using M-Mode echocardiography. TAPSE is a measure of right ventricular longitudinal function. Normal value is usually above 15 mm. It is a highly load dependent measure and optimal alignment of the ultrasound beam can be challenging.
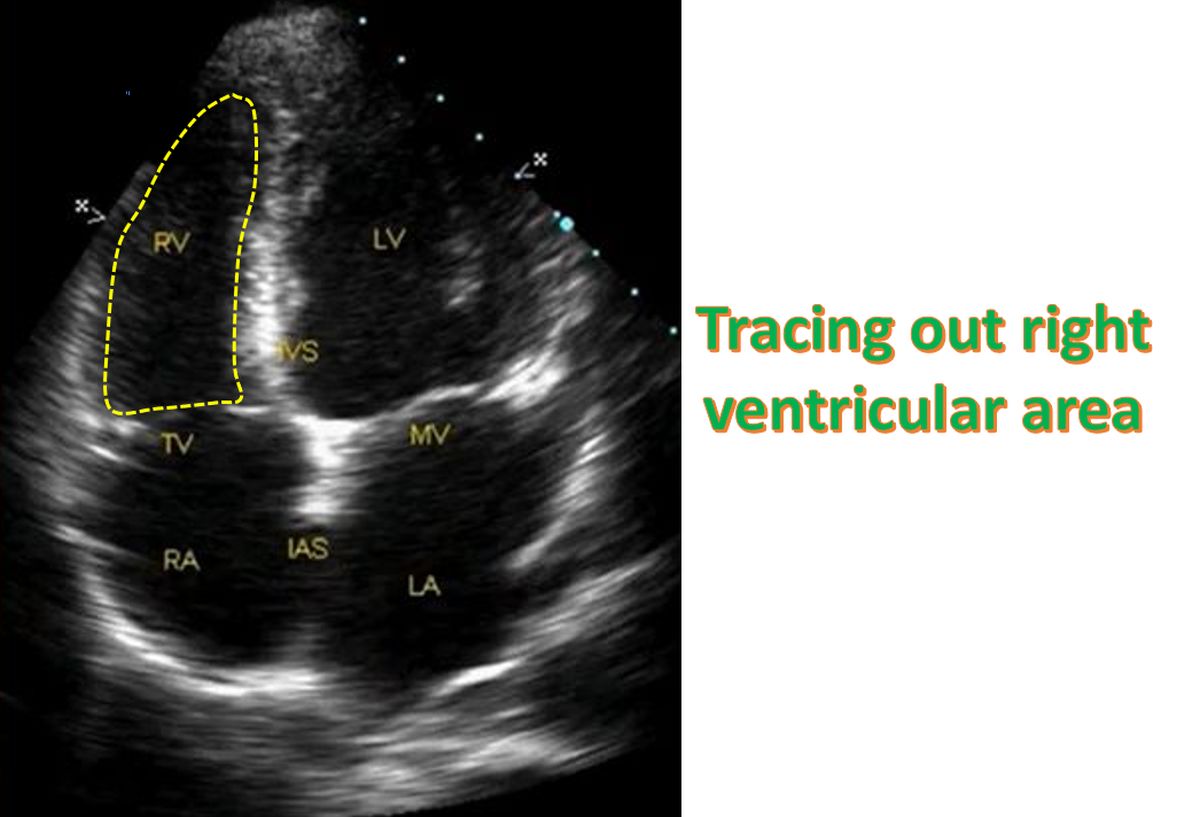
Right ventricular fractional area change can be measured from the four chamber view by tracing out the diastolic and systolic frames. Fractional area change (FAC) = (End diastolic area – End systolic area)/End diastolic area. Normal values range from 32-60%. Fractional area change is highly load dependent. Complex geometry of the right ventricle and the coarse trabeculations make tracing out the right ventricular area challenging. Still there has been good correlation with right ventricular ejection fraction measured using magnetic resonance imaging [2].
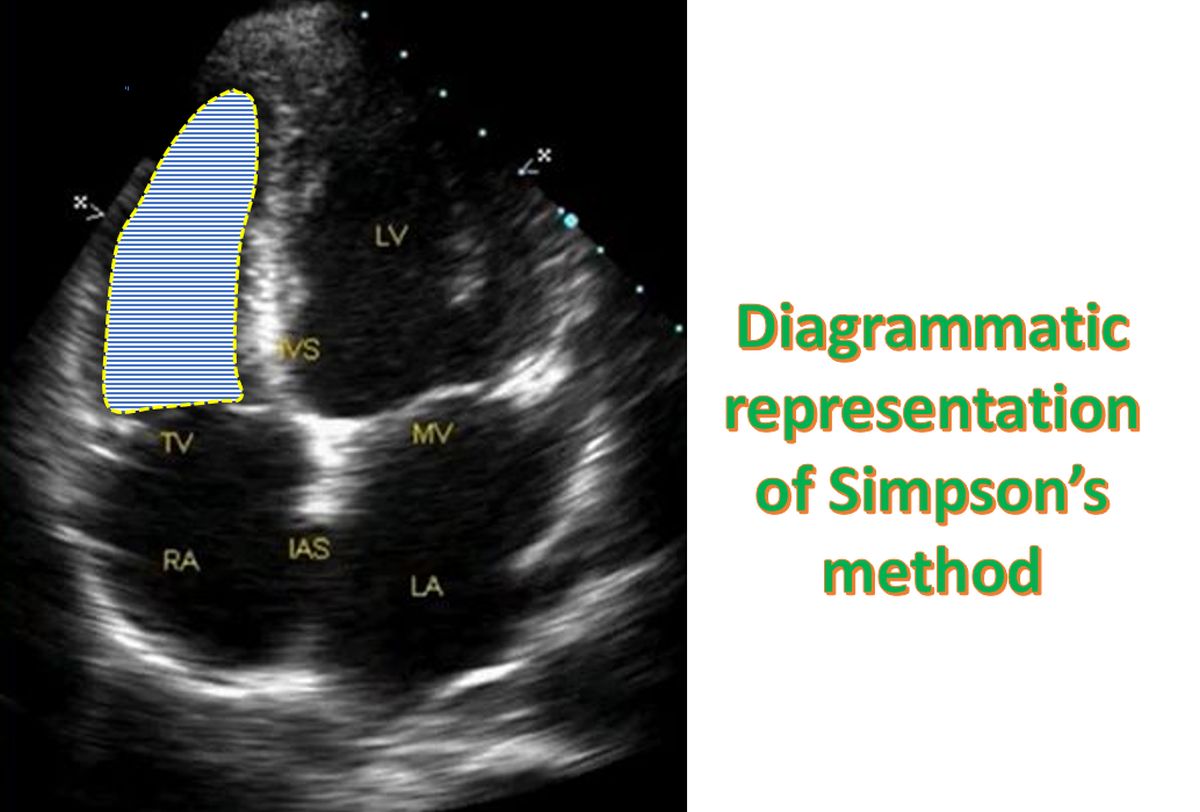
Right ventricular ejection fraction can be calculated using the Simpson’s rule. Right ventricular outline is traced out in systole and diastole as for left ventricular function evaluation by echocardiography, from the four chamber view. It has been shown to have prognostic value in heart failure, valvular heart disease and congenital heart disease. But it is highly load dependent and can be inaccurate in volume and pressure overload states. Precise measurement of right ventricular ejection fraction is often difficult due to the complex geometry of the right ventricle [2]. There are several limitations due to the geometry of the right ventricle.
Right ventricular diastolic function can be evaluated from the tricuspid inflow pattern by Doppler interrogation. Right ventricle can be an open system in diastole with antegrade forward flow into the pulmonary artery during atrial systole.
During Doppler evaluation of right ventricle, the 5-10% increase in the measurements with inspiration has to be considered. This is applicable to pulmonary artery systolic velocity, right ventricular gradient, tricuspid regurgitation velocity and tricuspid inflow Doppler. This may lead to inability to detect small changes in status of the right ventricle.
Right ventricular global function can be assessed by myocardial performance index. Myocardial performance index (MPI) is the ratio of the time spent in isovolumetric activity divided by the time spent in ventricular ejection [3].
MPI = (ICT + IRT) / ET
ICT: isovolumic contraction time; IRT: isovolumic relaxation time; ET: ejection time
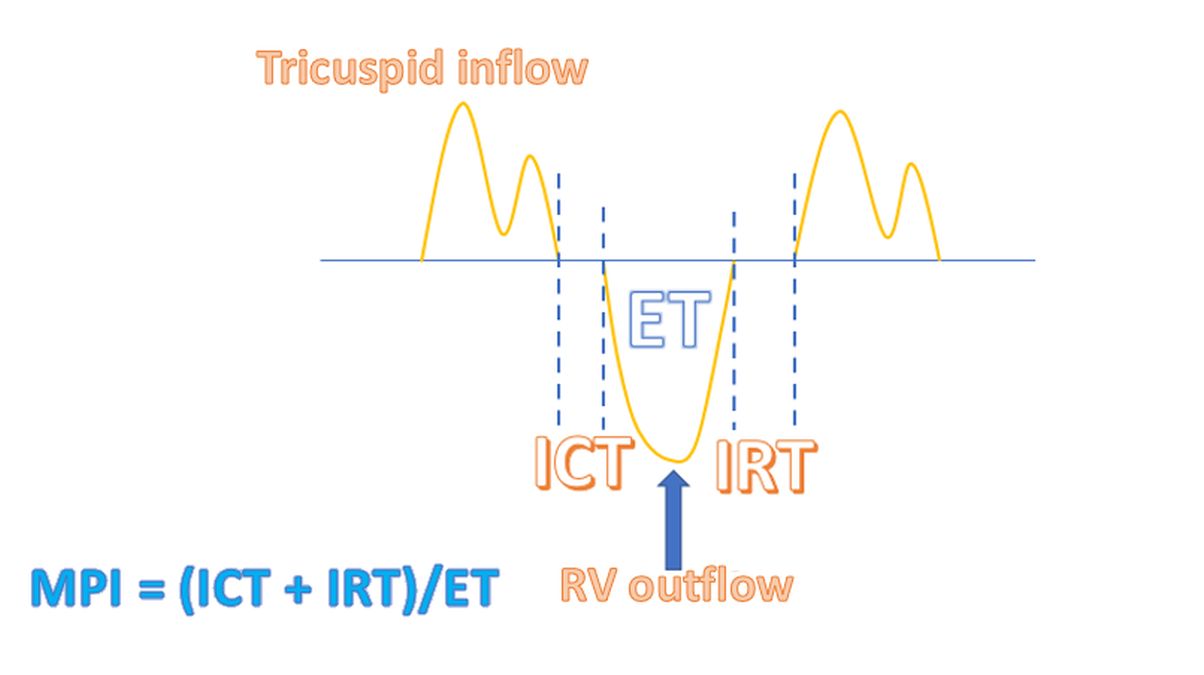
Myocardial performance index (Tei index) has an inverse relation with global ventricular function in that increasing values indicate worsening global ventricular function. There is good correlation between Doppler derived myocardial performance index and cath derived invasive measures as well as with the clinical outcome. Myocardial performance index has different normal ranges for different age groups and for the left and right ventricles, though it is roughly a little more than one third. Advantages of myocardial performance index are that it is simple to estimate, reproducible, not affected by geometry and assesses global function. Down sides of MPI are the non-simultaneous acquisition, load dependence, variation with heart rate, age and body surface area, and rhythm as well as non-specific being unable to differentiate between systolic and diastolic dysfunction. There could also be pseudo-normalization due to this.
Tei index can also be measured indirectly from the tissue Doppler. It is designated as tMPI [4]. Corresponding measurements on tissue Doppler are tIVCT: tissue isovolumic contraction time, tIVRT: tissue isovolumic relaxation time and tET: tissue ejection time. Measurements are taken using pulsed tissue Doppler from the lateral tricuspid annulus.
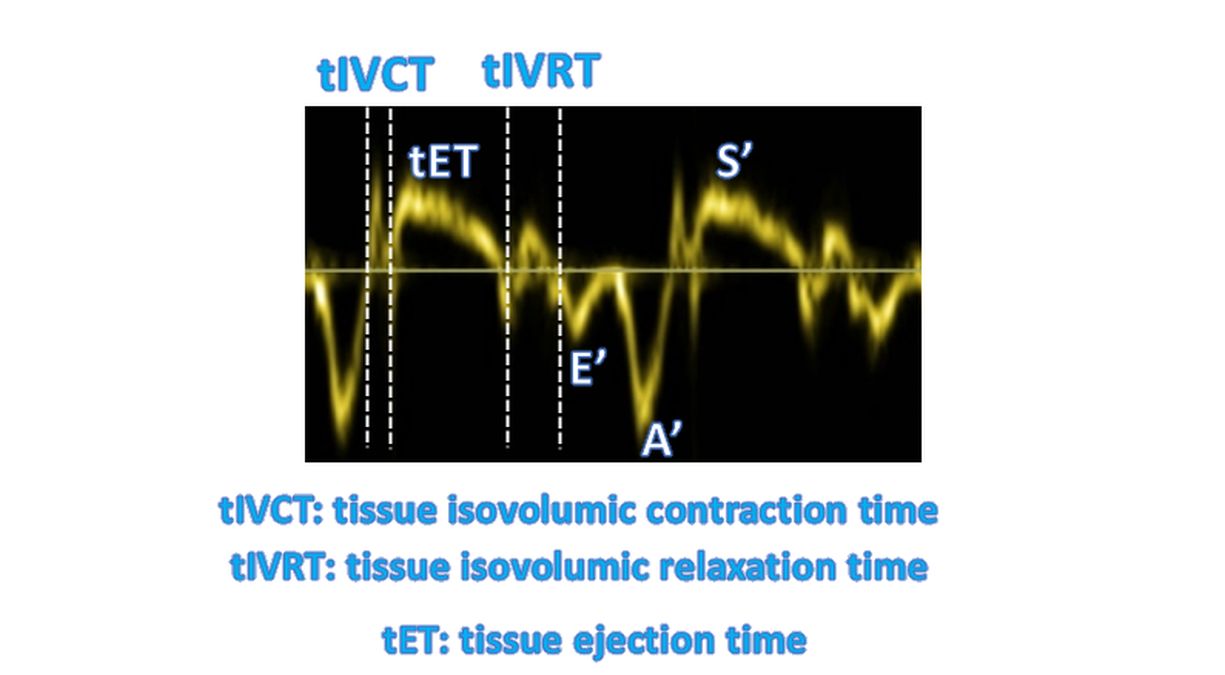
Longitudinal function of the right ventricle can be quantified by tissue Doppler methods [5]. Longitudinal velocities assessed by tissue Doppler techniques are the lateral mitral annulus velocity, septal annulus velocity and the tricuspid annulus velocity. These tracings have distinct E and A in diastole, a systolic velocity and spikes for isovolumetric contraction and relaxation. Tissue Doppler can quantify both systolic and diastolic myocardial function and is less load dependent. Early identification of right ventricular dysfunction and correlation with clinical function is feasible. Tissue Doppler technique can also assess radial function. Limitations of tissue Doppler include the angle dependence and confounding effects of cardiac tethering and translation.
Regional function of the right ventricle can be noted by strain and strain rate imaging [5]. Strain and strain rate imaging can also quantify both systolic and diastolic myocardial function and is less load dependent. Early identification of right ventricular dysfunction and correlation with clinical function is feasible as in the case of tissue Doppler imaging. Limitations of strain and strain rate imaging include the angle dependence, load dependence, aliasing and problems with high frame rates and data analysis.
Reference
- Singbal Y, Vollbon W, Huynh LT, Wang WY, Ng AC, Wahi S. Exploring Noninvasive Tricuspid dP/dt as a Marker of Right Ventricular Function. Echocardiography. 2015 Sep;32(9):1347-51. doi: 10.1111/echo.12877. Epub 2015 Jan 2. PMID: 25556710.
- Mahmood F, Shernan SK. Perioperative transoesophageal echocardiography: current status and future directions. Heart. 2016 Aug 1;102(15):1159-67. doi: 10.1136/heartjnl-2015-307962. Epub 2016 Apr 5. PMID: 27048769.
- Bleeker GB, Steendijk P, Holman ER, Yu CM, Breithardt OA, Kaandorp TA, Schalij MJ, van der Wall EE, Nihoyannopoulos P, Bax JJ. Assessing right ventricular function: the role of echocardiography and complementary technologies. Heart. 2006 Apr;92 Suppl 1:i19-26.
- Zimbarra Cabrita I, Ruisanchez C, Dawson D, Grapsa J, North B, Howard LS, Pinto FJ, Nihoyannopoulos P, Gibbs JS. Right ventricular function in patients with pulmonary hypertension; the value of myocardial performance index measured by tissue Doppler imaging. Eur J Echocardiogr. 2010 Sep;11(8):719-24. doi: 10.1093/ejechocard/jeq051. Epub 2010 Apr 21. PMID: 20410189.
- Pietrzak R, Werner B. Right ventricular function assessment using tissue Doppler imaging and speckle tracking echocardiography. J Ultrason. 2014 Sep;14(58):328-38. doi: 10.15557/JoU.2014.0033. Epub 2014 Sep 30. PMID: 26674180; PMCID: PMC4579681.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal