Atrial flutter ECG
Atrial flutter ECG


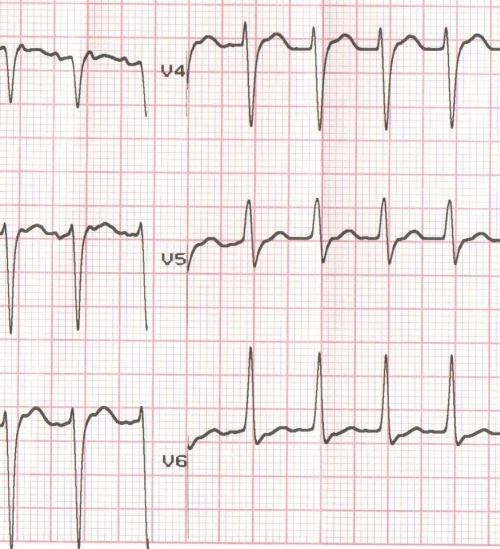
Positive flutter waves (F waves) are seen in inferior leads with 2:1 conduction. One flutter wave is seen within the ST segment and another in the usual location of a P wave. At one look, it looks like a reverse typical atrial flutter.
Comment by Dr. KKN Namboodiri:
I also feel it looks like reverse typical as per F wave morphology. But it could very well be a flutter circuit not involving the cavo-tricuspid isthmus (CTI). This is actually more likely if we go by statistics. As we know, Flutter morphology predominantly depends on whether posterior left atrium (LA) is activated caudocranially or craniocaudally, and right atrial (RA) activation has limited role in deciding it even in circuits limited to RA. In an RA flutter, the LA activation sequence depends on preferential activation through lower (coronary sinus – CS) or upper (Bachman Bundle) interatrial connections. In a counterclockwise flutter the activation reaches LA primarily through lower CS connections (when it exits in a counterclockwise direction across CTI to CS os region) and few other RA tachycardias can mimic this. Hence this morphology is characteristic of counter clockwise (CCW) loop of activation. But many other circuits, CTI CW flutter, upper RA circuits, upper LA circuits/focus can mimic this easily, and these are statistically more common. A low F amplitude, longer isoelectric interval, structural heart disease (SHD)/ myopathic illness (low QRS voltage in limb leads may suggest so in this case) and purely positive F in V1- all these markers may act as a few pointers towards LA flutter on a broader base. A longer cycle length (CL) also would do so (a softer point). Approach wise, we usually take all CTI-independent flutters on 3D now-a-days as it makes a big difference. Or in other words, a flutter having morphology other than CCW flutter. I am comfortable with 3D mapping in these cases as it gives a lot more additional information: 1. Idea about substrate, scar etc. 2. Extent of circuits 3. Completion of ablation, as no definite end point like CTI bidirectional block is not valid here.
CW RA flutter mimics CCW mitral isthmus dependent flutters and vice-versa!!
Thank you Dr. Namboodiri, for these detailed comments which have added a lot to its value.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal