Atrial functional mitral regurgitation
Atrial functional mitral regurgitation
Atrial functional mitral regurgitation occurs secondary to left atrial disease, without left ventricular dilatation and intrinsic mitral valve disease. Atrial functional MR typically occurs in the setting of long-standing atrial fibrillation. It is associated with increased mortality risk and hospitalization for heart failure [1]. Reported prevalence of atrial functional MR in patients with AF vary between 3 to 15%. These patients have worse clinical outcome [2].
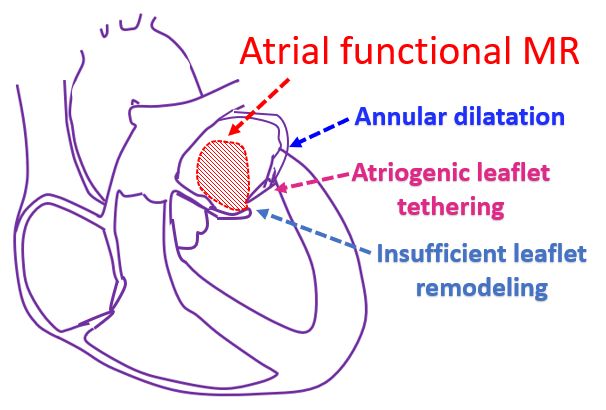
Dilatation of the mitral annulus, atriogenic tethering of mitral leaflets and insufficient mitral leaflet remodeling are thought to be important pathogenic mechanisms of atrial functional MR. Insufficient leaflet remodeling leads to annulus to leaflet area imbalance. In addition, reduced annular contractility, increased valve stress by flattened saddle shape of the annulus and left atrial dysfunction may be important triggers for atrial functional MR [2].
Evidence for atrial functional MR in atrial fibrillation was provided by a retrospective study of patients undergoing first AF ablation. Of the 828 patients screened, those with echocardiogram at the time of ablation and at one year clinical follow up were included. The study cohort of 53 patients had at least moderate MR. A reference cohort of 53 patients was randomly selected from 660 patients with mild or less MR. The effect of restoration of sinus rhythm was assessed by follow up echocardiogram [3].
It was observed that MR patients were older than controls and more often had persistent AF (62% vs 32%). Patients with MR had larger left atria, but similar left ventricular size and ejection fraction. Patients in continuous sinus rhythm had greater reductions in left atrial size and annular dimension. They had lower rates of significant mitral regurgitation, 24% vs 82%. Study authors concluded that AF can result in atrial functional MR and that it improves if sinus rhythm is restored.
Surgical considerations of atrial functional MR are different from ventricular functional MR [1]. Surgical treatment is currently the most reliable option for atrial functional MR [2].
A retrospective study analyzed 10 patients with chronic AF who underwent mitral valve repair for atrial functional MR. All had chronic heart failure symptoms and at least one prior admission for heart failure complicating severe MR. Ring annuloplasty was performed in all patients. Concomitant tricuspid valve repair was also done in all patients. There was no mortality or re-admission due to heart failure during a follow up of 10-52 months [4].
MR at the most recent examination was mild or improved in degree in all patients. Left atrial volume index decreased and New York Heart Association functional class improved dramatically.
Mitral valve adaptation to isolated annular dilatation in atrial functional MR due to AF has been evaluated by three dimensional echocardiography. Of the 86 patients in the study, 53 had nonvalvular persistent AF without left ventricular dysfunction or dilatation. 33 were normal controls. Total mitral leaflet area (MLA) was 22% larger in AF patients than in controls [5].
As annular area (AA) increased, adaptive indices MLA/AA ratio and MLA to closure area plateaued. MR increased as the ratio of MLA to closure area decreased. Though the posterior to anterior MLA ratio remained constant, posterior to anterior mitral annulus perimeter increased. Multivariate determinants of MR were annular area, total MLA to closure area and posterior to anterior perimeter ratios [5].
The study authors concluded that MLA increases in AF with isolated annular dilatation and normal left ventricular function. The compensatory leaflet enlargement becomes insufficient with greater annular enlargement. Leaflets fail to match the asymmetrical annular remodeling and increases MR.
Catheter based interventions like transcatheter edge-to-edge repair (TEER) has been used for atrial functional MR. Various devices to mimic surgical annuloplasty are being developed for the treatment of atrial functional MR. Theoretically, annuloplasty devices are expected to be more effective for annulus area to leaflet area imbalance. As these patients tend to be older and with comorbidities, catheter based treatment might become the treatment of choice for atrial functional MR [2].
Clinical outcomes with TEER in atrial functional MR from the EXPAND (A Contemporary, Prospective, Multi-Center Study Evaluating Real-World Experience of Performance and Safety for the Next Generation of MitraClip Devices) registry has been reported. 53 patients in the EXPAND registry had atrial functional secondary MR and 360 patients had ventricular secondary MR. In the atrial functional MR cohort, TEER resulted in a significant reduction in MR through one year, with MR grade 2 or less in all patients. Kansas City Cardiomyopathy Questionnaire score and functional class improved at one year follow up [6].
Another retrospective study had 118 patients of atrial functional MR. Technical success of TEER was 94.1% and MR reduction to 1+ or less was achieved in 94 cases. In-hospital mortality was 2.5%. In multivariable analysis, a large left atrial volume index and low leaflet to annulus index were associated with a lower incidence of MR reduction to 1+ or less after TEER for atrial functional secondary MR [7].
References
- Fan Y, Wan S, Wong RH, Lee AP. Atrial functional mitral regurgitation: mechanisms and surgical implications. Asian Cardiovasc Thorac Ann. 2020 Sep;28(7):421-426. doi: 10.1177/0218492320941388. Epub 2020 Jul 1. PMID: 32611195.
- Kagiyama N, Mondillo S, Yoshida K, Mandoli GE, Cameli M. Subtypes of Atrial Functional Mitral Regurgitation: Imaging Insights Into Their Mechanisms and Therapeutic Implications. JACC Cardiovasc Imaging. 2020 Mar;13(3):820-835. doi: 10.1016/j.jcmg.2019.01.040. Epub 2019 Aug 14. PMID: 31422123.
- Gertz ZM, Raina A, Saghy L, Zado ES, Callans DJ, Marchlinski FE, Keane MG, Silvestry FE. Evidence of atrial functional mitral regurgitation due to atrial fibrillation: reversal with arrhythmia control. J Am Coll Cardiol. 2011 Sep 27;58(14):1474-81. doi: 10.1016/j.jacc.2011.06.032. PMID: 21939832.
- Takahashi Y, Abe Y, Sasaki Y, Bito Y, Morisaki A, Nishimura S, Shibata T. Mitral valve repair for atrial functional mitral regurgitation in patients with chronic atrial fibrillation. Interact Cardiovasc Thorac Surg. 2015 Aug;21(2):163-8. doi: 10.1093/icvts/ivv119. Epub 2015 May 16. PMID: 25980774.
- Kim DH, Heo R, Handschumacher MD, Lee S, Choi YS, Kim KR, Shin Y, Park HK, Bischoff J, Aikawa E, Song JM, Kang DH, Levine RA, Song JK. Mitral Valve Adaptation to Isolated Annular Dilation: Insights Into the Mechanism of Atrial Functional Mitral Regurgitation. JACC Cardiovasc Imaging. 2019 Apr;12(4):665-677. doi: 10.1016/j.jcmg.2017.09.013. Epub 2017 Dec 13. PMID: 29248661; PMCID: PMC5993562.
- Sodhi N, Asch FM, Ruf T, Petrescu A, von Bardeleben S, Lim DS, Maisano F, Kar S, Price MJ. Clinical Outcomes With Transcatheter Edge-to-Edge Repair in Atrial Functional MR From the EXPAND Study. JACC Cardiovasc Interv. 2022 Sep 12;15(17):1723-1730. doi: 10.1016/j.jcin.2022.07.023. PMID: 36075643.
- Tanaka T, Sugiura A, Öztürk C, Vogelhuber J, Tabata N, Wilde N, Zimmer S, Nickenig G, Weber M. Transcatheter Edge-to-Edge Repair for Atrial Secondary Mitral Regurgitation. JACC Cardiovasc Interv. 2022 Sep 12;15(17):1731-1740. doi: 10.1016/j.jcin.2022.06.005. Epub 2022 Aug 22. PMID: 36075644.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal