Atrial repolarization wave
Atrial repolarization wave
Atrial repolarization wave – Ta wave
(Representative image)
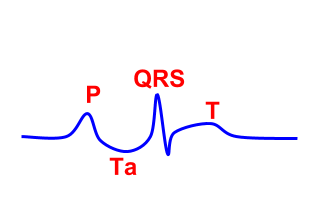
Atrial repolarization wave (Ta wave) is usually not evident on the electrocardiogram (ECG) as it has a low amplitude of hundred to two hundred microvolts and is usually hidden in the QRS complex. [1] It can also extend into the ST segment causing ST segment depression mimicking myocardial ischemia, especially during an exercise test. This can cause a false positive response. But this type of response can be identified by the associated depression of the PR segment so that the PR segment along with the ST segment forms a parabola, unlike the broken parabola pattern seen with true ischemic ST segment depression. The exercise time will be longer, more than six minutes, there will be no associated chest pain, and the peak exercise heart rate achieved is higher than one hundred and twenty five beats. Slavich G et al noted the role of atrial repolarization in ST-segment depression during exercise as 5.5 percent.
To study Ta wave when it is not obscured by the QRS complex, independent P waves in complete heart block are evaluated. Holmqvist F and associates [2] did this analysis in forty patients. They recorded standard 12-lead ECGs and transformed them to orthogonal leads and studied the records using signal averaged P wave analysis. They noted that the Ta wave polarity was opposite to that of P wave in all leads and the mean Ta wave duration was about 320 milliseconds. This was in contrast with the mean P wave duration of about 120 milliseconds. They concluded that even though the peak of Ta wave may occur within the PQ segment during normal AV conduction, it may be difficult to differentiate between normal and abnormal atrial depolarization unless an algorithm for QRST cancellations is used.
A modified limb lead (MLL) system for detection of atrial repolarization on surface ECG has been devised by Sivaraman J et al [3]. This lead system is useful in detecting atrial repolarization on surface ECG, more so in case of complete heart block where the most of the atrial repolarization activity is not masked by ventricular activity [4]. In usual case, atrial repolarization is partly masked by the QRS complex and subsequent ventricular repolarization. A brief description of the MLL is available in a free full text IPEJ article [5].
References
- Slavich G et al. Pseudoischemic ST-segment due to atrial repolarization during exercise test. Review of the literature, diagnostic criteria and personal experience. G Ital Cardiol (Rome). 2006;7:670-4.
- Holmqvist F et al. Detailed ECG analysis of atrial repolarization in humans. Ann Noninvasive Electrocardiol. 2009;14:13-8.
- Sivaraman J, Uma G, Venkatesan S, Umapathy M, Dhandapani V.E. Normal limits of ECG measurements related to atrial activity using a modified limb lead system. Anatol J Cardiol.2015 Jan;15(1):2–6.
- Jayaraman S, Gandhi U, Sangareddi V, Mangalanathan U., Shanmugam R.M. Unmasking of atrial repolarization waves using a simple modified limb lead system. Anatol J Cardiol. 2015 Aug;15(8):605–610.
- Francis J. ECG monitoring leads and special leads. Indian Pacing Electrophysiol J. 2016 May-Jun; 16(3): 92–95.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal