Cardiac implantable electronic devices (CIED) on CXR
Cardiac implantable electronic devices (CIED) on CXR
Cardiac pacemakers where the earliest cardiac implantable electronic devices (CIED) to be used ever since the first implant in 1958.
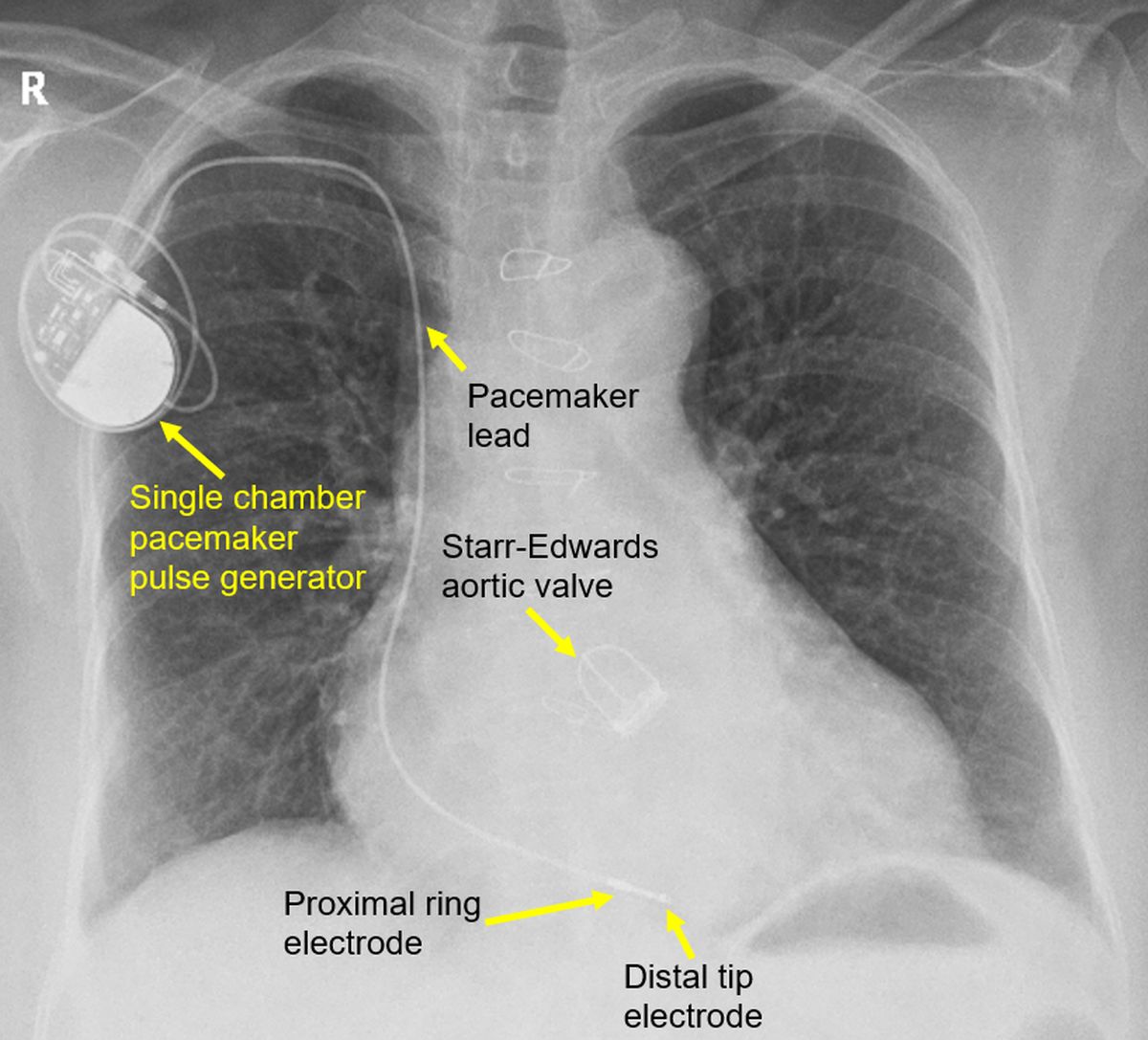
Single chamber pacemaker: Picture below shows a single chamber pacemaker with pulse generator and lead. Two electrodes for stimulation – a proximal ring electrode and distal tip electrode are seen towards the apex of the right ventricle. The pulse generator is seen in the right pectoral region. The lead is coursing through the right subclavian vein into the superior vena cava. From superior vena cava it reaches the right ventricle through the right atrium. A Starr-Edwards prosthetic aortic valve with three struts and sewing ring is also seen within the cardiac shadow.
Dual chamber pacemaker: Picture below shows a dual chamber pacemaker with a right atrial lead and a right ventricular lead.
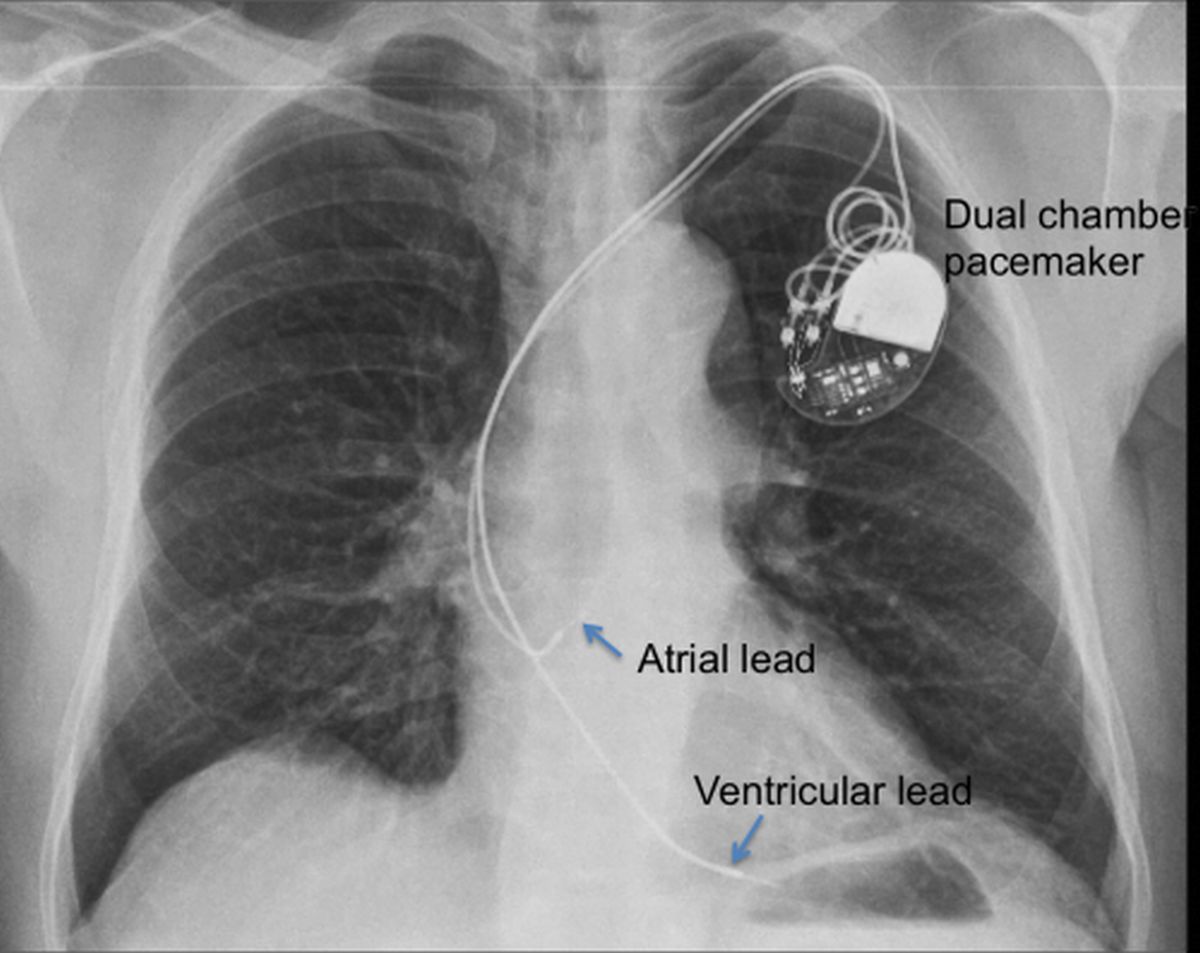
In this case, the pacemaker pulse generator was implanted in the left pectoral region. The leads traverse the left subclavian vein and left brachiocephalic vein to reach the superior vena cava. The atrial lead is a J shaped lead and tip is usually located in the right atrial appendage. The ventricular lead was placed at the right ventricular apex.
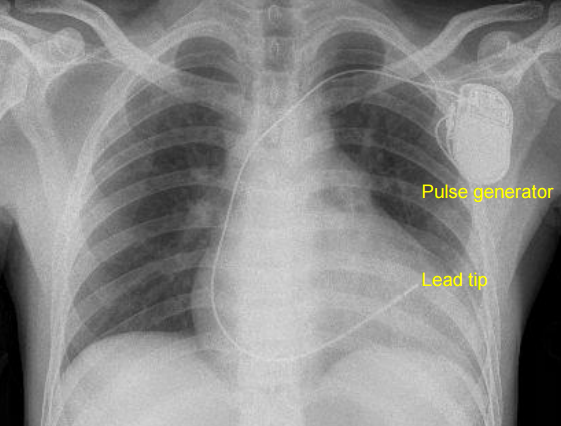
CXR in septal pacing: Picture given below shows a single chamber pacemaker with a screw in lead kept on the septal aspect of the right ventricle. Septal pacing on the right ventricular outflow region may give a narrower QRS complex with better left ventricular synchrony. A narrower QRS reduces the long term chance of left ventricular dysfunction, which is a down side of right ventricular apical pacing. It may be noted that lead tip is located higher than in the previous two cases.
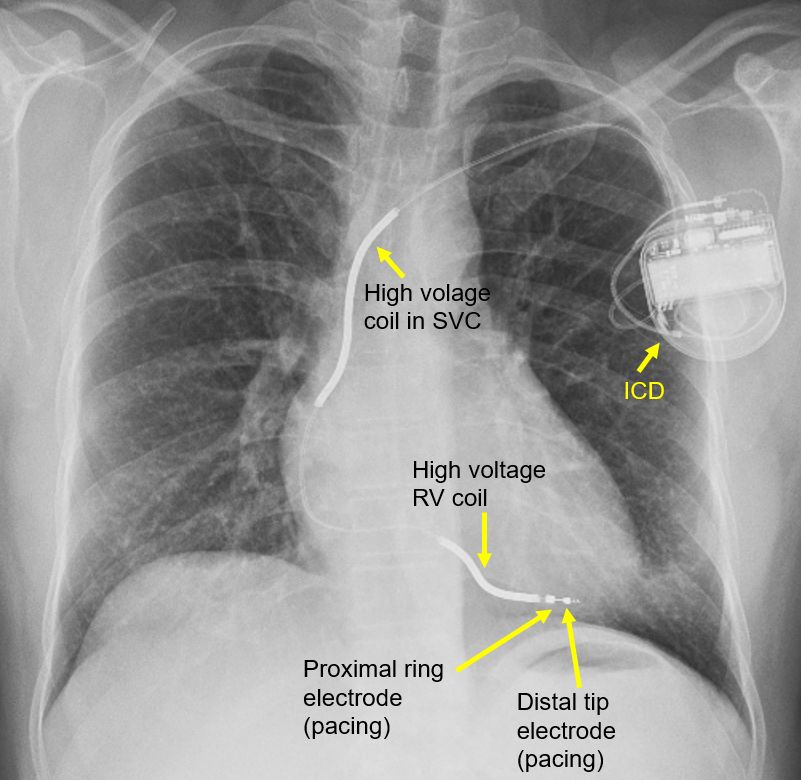
Implantable cardioverter defibrillator (ICD): ICD is an implantable device which can treat both brady and tachy arrhythmias. If it detects significant bradycardia, it gives back up pacing signals. If a ventricular tachycardia (fast rhythm originating from the lower chambers of the heart), it tries initially to suppress it by overdrive pacing (giving electrical signals at a rate higher than that of the tachycardia). If it does not succeed, a direct current internal shock is delivered across the high voltage coils to terminate the arrhythmia. If a very fast ventricular tachycardia which is life threatening or a ventricular fibrillation is detected, the device straight away gives a direct current shock to terminate the arrhythmia. Figure below shows the ICD with two high voltage coils (one in superior vena cava and another in right ventricle) and two pacing electrodes near the tip of the right ventricular lead. This is a single chamber ICD. A dual chamber ICD will have an additional atrial lead which is useful in sensing atrial arrhythmias and avoiding unnecessary shocks.
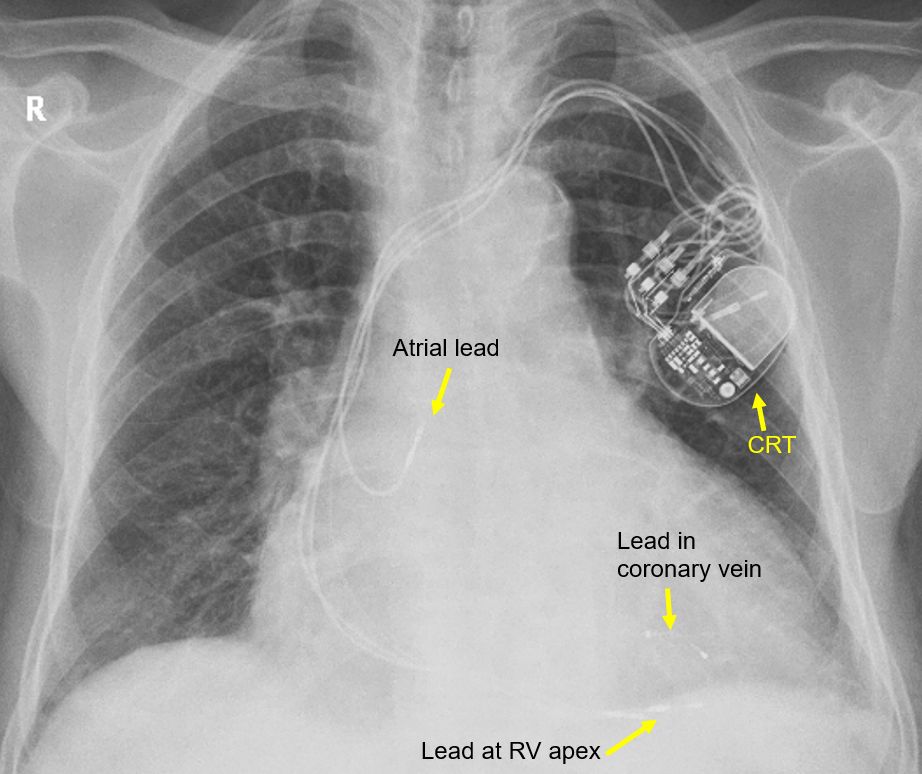
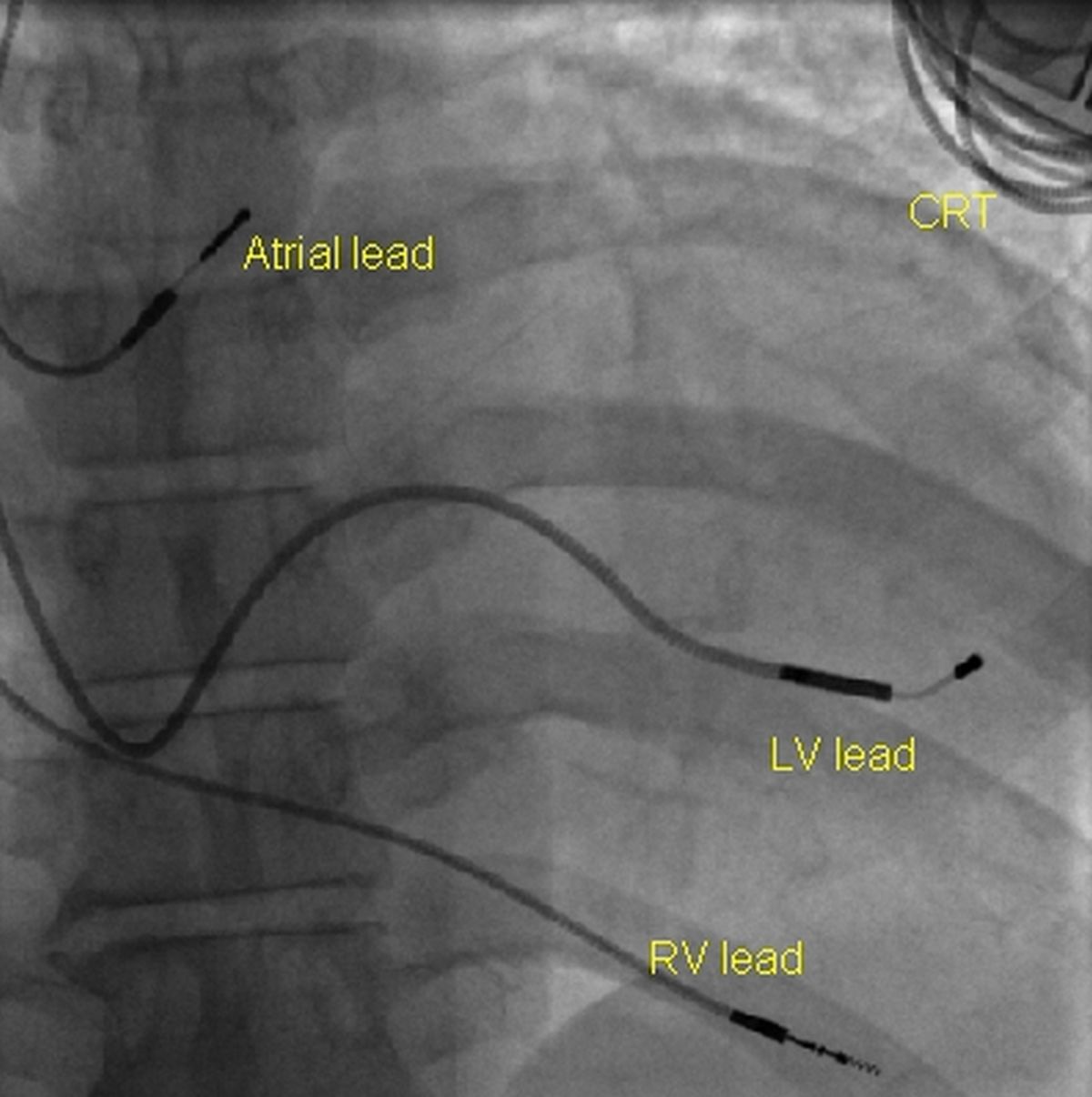
Cardiac resynchronization therapy (CRT): Cardiac resynchronization therapy is an advanced form of three chamber pacing which is used to synchronize left ventricular contraction in heart failure. Hence they are also known as heart failure devices. An ICD can be included in the device, then it will be called CRT-D (while the plain CRT will be called CRT-P). First picture shows a CRT-P device with one atrial lead and one lead each in the right ventricle and coronary vein (to pace the left ventricle epicardially). Second one shows the fluoroscopic view of three leads of a CRT-P. It shows an atrial lead, a right ventricular (RV) lead and a left ventricular lead (LV) in the coronary vein. Since it is a CRT-P, no high voltage leads are present. For CRT-D, the device will be larger as it requires a larger battery for delivering defibrillator shocks. In addition, two high voltage electrodes will be present, one placed in the superior vena cava and another in the right ventricle. CRT-D was also called a combo device as it was a combination of CRT and ICD.
Subcutaneous ICD: Subcutaneous ICD is a leadless ICD with a device implanted subcutaneously in the left infra axillary region. An electrode is placed subcutaneously on the left side of the sternum. The shock is delivered between the electrode and the body of the ICD can. Though it can deliver post shock bradycardia pacing for a short period, it cannot deliver overdrive pacing for a tachyarrhythmia.
Leadless pacemaker: Leadless pacemaker is a cylindrical capsule like device with structures to anchor it to the right ventricular wall. They do not have external leads and can be implanted through the femoral vein into the right ventricle.
Implantable loop recorder: While all the above were therapeutic devices, an implantable loop recorder (ILR) is a purely diagnostic device. It can be implanted subcutaneously in the infraclavicular region and will function up to three years. ILR is very useful in the detection of intermittent arrhythmias which are infrequent, but potentially dangerous.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal