Cardiology MCQs
Cardiology MCQs
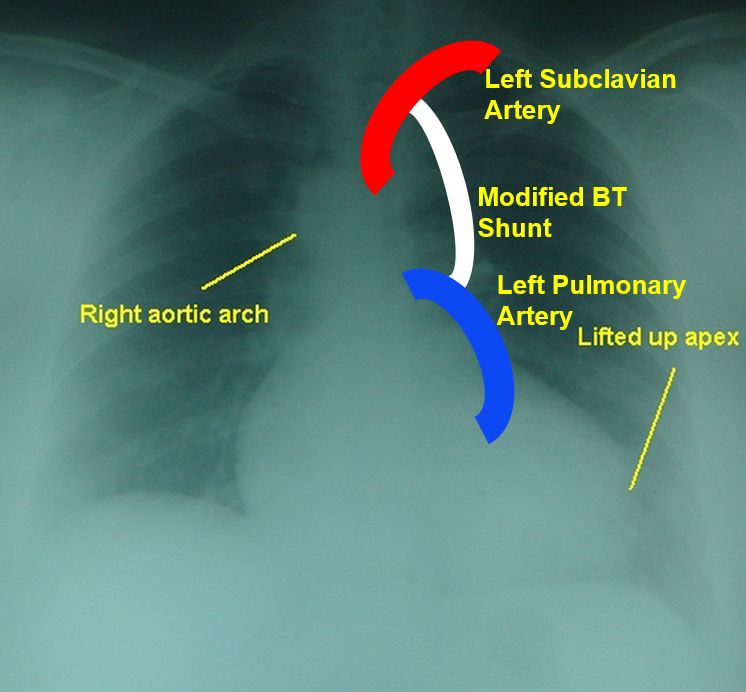
Modified Blalock-Taussig shunt is:
- End to side anastomosis of subclavian artery to a pulmonary artery
- Side to side anastomosis of main pulmonary artery to aorta
- Side to side anastomosis of subclavian artery to a pulmonary artery using a conduit
- Anastomosis of superior vena cava to right pulmonary artery
Correct answer: 3. Side to side anastomosis of subclavian artery to a pulmonary artery using a conduit
In classic Blalock-Taussig shunt, the subclavian artery is divided and anastomosed to the pulmonary artery as an end to side anastomosis. In modified Blalock – Taussig shunt, a Gore – Tex graft is used to connect the subclavian artery to the pulmonary artery. In Davidson shunt, a Gore-Tex graft is used to connect ascending aorta to main pulmonary artery [Tomasian A, Malik S, Shamsa K, Krishnam MS. Congenital heart diseases: post-operative appearance on multi-detector CT-a pictorial essay. Eur Radiol. 2009 Dec;19(12):2941-9]. Glenn shunt connects the superior vena cava to right pulmonary artery.
Complication of Fontan procedure:
- Plastic bronchitis
- Protein losing enteropathy
- Heart failure
- All of the above
- None of the above
Correct answer: 4. All of the above
Heart failure was the mode of death in 34% in a series of 600 adult Fontan survivors. Arrhythmia or sudden death was the reason in 24% [Ohuchi H, Inai K, Nakamura M, Park IS, Watanabe M, Hiroshi O, Kim KS, Sakazaki H, Waki K, Yamagishi H, Yamamura K, Kuraishi K, Miura M, Nakai M, Nishimura K, Niwa K; JSACHD Fontan Investigators. Mode of death and predictors of mortality in adult Fontan survivors: A Japanese multicenter observational study. Int J Cardiol. 2019 Feb 1;276:74-80]. Protein losing enteropathy is an important complication of Fontan circulation. Atrioventricular valve regurgitation is often associated with ventricular failure and it can be progressive. Pleural effusion, chylothorax and plastic bronchitis are important pulmonary complications associated with Fontan circulation. Predisposition to thrombosis and thromboembolism are also well known. It contributed to 7.9% of the late deaths in one study [Khairy P, Fernandes SM, Mayer JE Jr, Triedman JK, Walsh EP, Lock JE, Landzberg MJ. Long-term survival, modes of death, and predictors of mortality in patients with Fontan surgery. Circulation. 2008 Jan 1;117(1):85-92].
Gold standard for myocardial viability:
- Systolic thickening of myocardial segment on echocardiography
- Absence of late gadolinium enhancement on magnetic resonance imaging
- Preserved metabolic activity on positron emission tomography
- Myocardial scar detected on multidetector computed tomography
Correct answer: 3. Preserved metabolic activity on positron emission tomography
Preserved metabolic activity on positron emission tomography is considered the gold standard in myocardial viability assessment. [Tamaki N, Kawamoto M, Tadamura E, Magata Y, Yonekura Y, Nohara R, Sasayama S, Nishimura K, Ban T, Konishi J. Prediction of reversible ischemia after revascularization. Perfusion and metabolic studies with positron emission tomography. Circulation. 1995 Mar 15;91(6):1697-705]. Segmental thickening and absence of scarring detected by other imaging modalities are also useful indicators of viability.
Wrong statement about coronary subclavian steal syndrome:
- Occurs after CABG using left internal mammary artery (LIMA)
- Diversion of blood flow from coronary circulation to exercising left upper limb
- High grade stenosis or occlusion of left subclavian artery distal the origin of LIMA
- Can manifest with angina
Correct answer: 3. High grade stenosis or occlusion of left subclavian artery distal the origin of LIMA
Coronary subclavian steal syndrome occurs when there is a high grade stenosis or occlusion of left subclavian artery proximal to the origin of the LIMA. Cardiovascular manifestation of coronary subclavian steal syndrome could be angina, myocardial infarction, malignant arrhythmias or heart failure [Cua B, Mamdani N, Halpin D, Jhamnani S, Jayasuriya S, Mena-Hurtado C. Review of coronary subclavian steal syndrome. J Cardiol. 2017 Nov;70(5):432-437]. Cerebral symptoms can occur due to steal from the cerebral circulation through the vertebral artery.
Which of the following is NOT a usual feature of acute aortic regurgitation?
- Long and loud diastolic murmur
- Mitral valve preclosure
- Peripheral signs of AR not seen
- Diastolic mitral regurgitation may occur
Correct answer: 1. Long and loud diastolic murmur
The classical decrescendo early diastolic murmur and peripheral signs of chronic aortic regurgitation are not features of acute AR. An early diastolic murmur if it is heard, is usually softer and shorter in acute AR. High left ventricular diastolic pressure causes mitral valve preclosure. But when the left ventricular diastolic pressure becomes very high in severe acute AR, mitral valve reopens in late diastole, causing diastolic mitral regurgitation [Hamirani YS, Dietl CA, Voyles W, Peralta M, Begay D, Raizada V. Acute aortic regurgitation. Circulation. 2012 Aug 28;126(9):1121-6].
Which was the phase 3 trial of Selexipag, a drug for treatment of pulmonary hypertension?
- TASTE trial
- PRAMI trial
- GRIPHON trial
- VITAL trial
Correct answer: 3. GRIPHON Trial
TASTE trial was Thrombus Aspiration during ST-Segment Elevation Myocardial Infarction. PRAMI was Preventive Angioplasty in Myocardial Infarction. VITAL trial was on role of vitamin D in cardiovascular disease. [Prostacyclin (PGI2) Receptor Agonist In Pulmonary Arterial Hypertension (GRIPHON) study: Sitbon O, Channick R, Chin KM, Frey A, Gaine S, Galiè N, Ghofrani HA, Hoeper MM, Lang IM, Preiss R, Rubin LJ, Di Scala L, Tapson V, Adzerikho I, Liu J, Moiseeva O, Zeng X, Simonneau G, McLaughlin VV; GRIPHON Investigators. Selexipag for the Treatment of Pulmonary Arterial Hypertension. N Engl J Med. 2015 Dec 24;373(26):2522-33].
Wrong statement about third heart sound:
- In mitral regurgitation S3 need not indicate left ventricular dysfunction
- S3 occurs just after the opening of the atrioventricular valve
- It is due to rapid acceleration of transmitral blood flow as the ventricles fill
- It corresponds in timing to shortly after the peak of the early diastolic E wave of transmitral flow
Correct answer: 3. It is due to rapid acceleration of transmitral blood flow as the ventricles fill
Third heart sound (S3) occurs in early diastole due to rapid deceleration of transmitral blood flow as the ventricles fill [Manson AL, Nudelman SP, Hagley MT, Hall AF, Kovács SJ. Relationship of the third heart sound to transmitral flow velocity deceleration. Circulation. 1995 Aug 1;92(3):388-94].
Takayasu arteritis is an inflammatory disorder affecting aorta and its major branches. Takayasu was:
- Vascular surgeon
- Ophthalmologist
- Physician
- Cardiologist
Correct answer: 2. Ophthalmologist
Takayasu was an ophthalmologist, who noted characteristic fundal arteriovenous anastomoses in a young female in 1905 and published it in Acta of the Opthalmic Society of Japan in 1908 (12:554–5). Onishi and Kagosha described similar cases associated with absent radial pulses in the same year [Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. J Clin Pathol. 2002 Jul;55(7):481-6].
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal