Closed loop catheter position in PDA with video
Closed loop catheter position in PDA
Fluoroscopy video
Angiographic video -posteroanterior (PA) and lateral views demonstrating the closed loop catheter position. The catheter is seen coursing down the descending aorta well below the diaphragm.
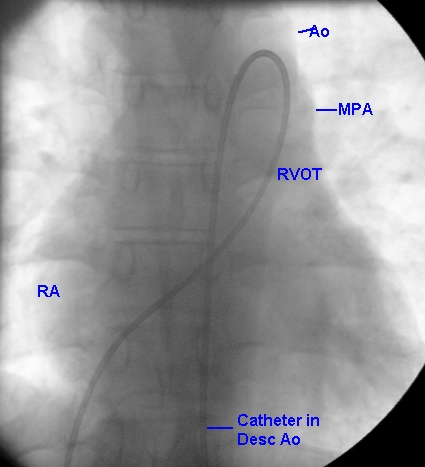
The catheter is seen emerging from the inferior vena cava into the right atrium (RA) above the right hemidiaphragm and crossing the mid line across the tricuspid valve into the right ventricle. In the right ventricle, it does not go into the apical region, but goes straight to the right ventricular outflow (RVOT) region. From the RVOT it crosses the pulmonary valve into the main pulmonary artery (MPA). From the MPA, it enters the descending aorta through the PDA which is situated at the junction of the left pulmonary artery and the MPA. Ao: aorta; Desc Ao: descending aorta. The closed loop catheter position in PDA has to be differentiated from the open loop catheter position which occurs in aortopulmonary window. In aortopulmonary window, the catheter enters the ascending aorta to the right of the main pulmonary artery without curving further to the left as in PDA. This produces an open loop appearance rather than a closed loop appearance. Open loop appearance can also rarely be seen in PDA, especially in slightly tilted views when the pulmonary artery is dilated.
When a right heart catheter passes from main pulmonary artery down the lung fields, it could be either in the left pulmonary artery or the descending aorta. If it passes very close to the left border of the spine, it is more likely to be in the descending aorta. A more definite way to confirm that it is in the aorta is to pan the table so that the course of the catheter dipping below the diaphragm can be documented as in this image. Catheter tip pressure tracing is helpful when the pulmonary arterial pressures are not elevated as the pressure rises abruptly on entering the aorta from the pulmonary artery. But in severe pulmonary hypertension as in a large PDA, the pulmonary and aortic pressures may be nearly equal. Another way to confirm is to draw out a sample of blood and check the oxygen saturation, which will be higher in the aorta. There can be a problem in this case also, if there is a right to left shunt across the ductus. Hence the usual method of confirmation is simply by panning the table to see that the catheter tip can be passed below the level of the diaphragm.
Lateral view of the fluoroscopic image shows the catheter emerging from the inferior vena cava into the right atrium above the right hemidiaphragm. The anterior course of the catheter documents its position in the right ventricle (RV), which is just beneath the sternum. The catheter further curves posteriorly as it crosses the pulmonary artery into the PDA. The location of the PDA is identified by the overlapping tracheal air column. Further the catheter passes down in the descending aorta which has a course adjacent to the spine. In the lateral view also, the course below the diaphragm can be documented by moving the table up and showing the catheter tip.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal