Coronary angiographic views
Coronary angiographic views
Coronary angiography is done in multiple projections or views to get a three dimensional idea of the coronary lesions. Some regions of the coronary arteries may appear foreshortened in certain views so that true length of the lesion may not be appreciated. Actual severity of eccentric stenosis can be ascertained only by multiple orthogonal views. Even though there are several conventional views for coronary angiography, unusual angulations may be needed in an individual case to guide coronary interventions. Often a test shot is given before the actual cine run to see if the branches are overlapping or not.
Common projections used in coronary angiography are left anterior oblique (LAO), right anterior oblique (RAO), postero-anterior (PA or AP), and lateral views. In addition to these, varying degrees of cranial or caudal angulations can be added to these views. In general, proximal parts of the major vessels are best seen in caudal projections.
Views for left coronary angiography
Spider view or LAO caudal view is often the first view taken during coronary angiography. This view is useful in visualising the left main coronary artery and its bifurcation into left anterior descending (LAD) coronary artery and left circumflex (LCX) coronary artery. LAO angulation may vary from 40-50º and caudal angulation 25-40º [1].
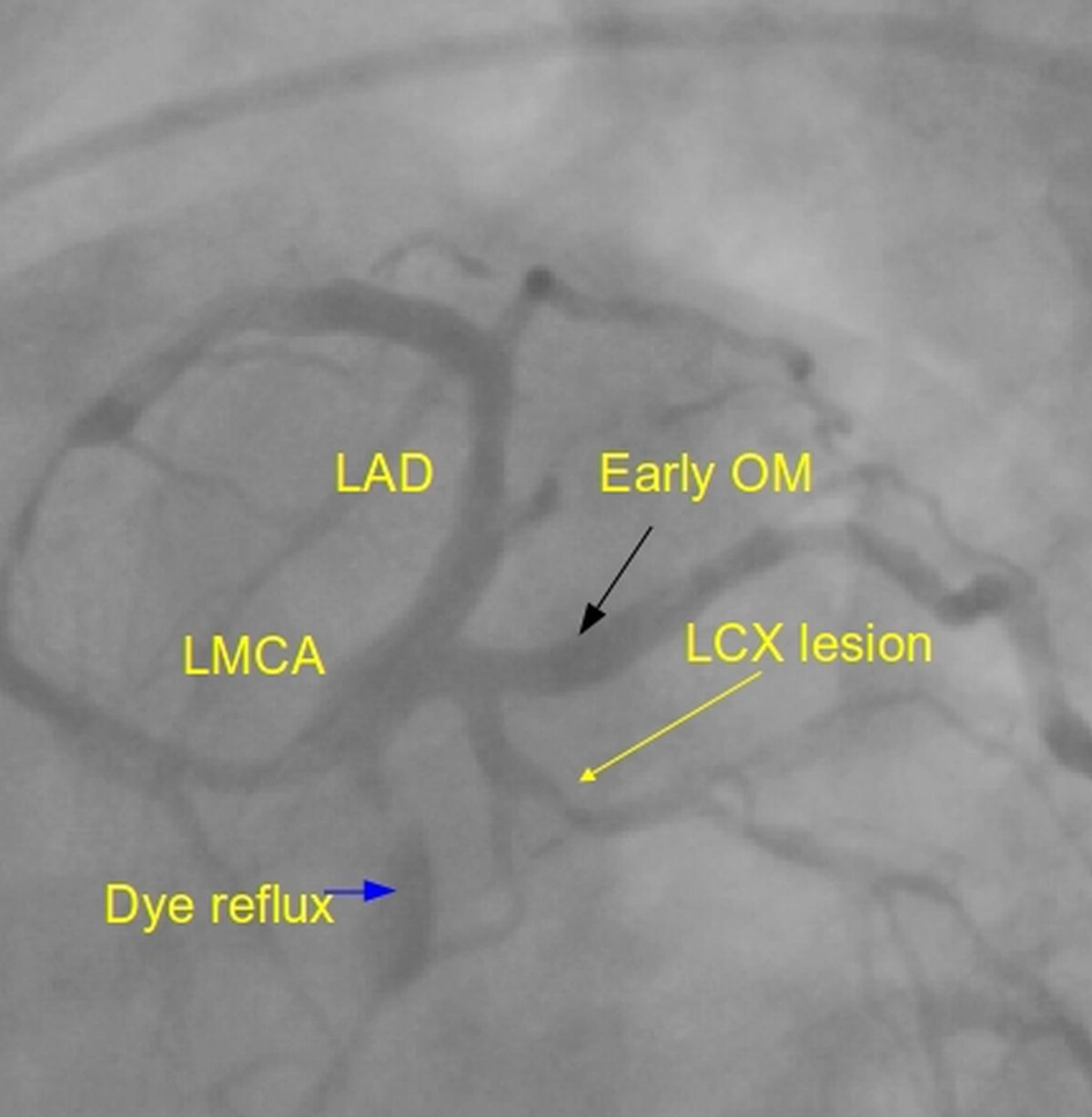
LAO caudal view of left coronary angiogram resembles a spider and hence the term spider view. LMCA: left main coronary artery; LCX: left circumflex coronary artery (lesion in LCX marked by yellow arrow); LAD: left anterior descending coronary artery; Early OM: early obtuse marginal branch of the LCX. From the LMCA bifurcation, LAD is seen towards the catheter side and LCX towards the opposite side in this view. Dye (contrast) reflux into the aorta from LMCA is seen. Absence of dye reflux would mean left main ostial disease or rarely spasm.
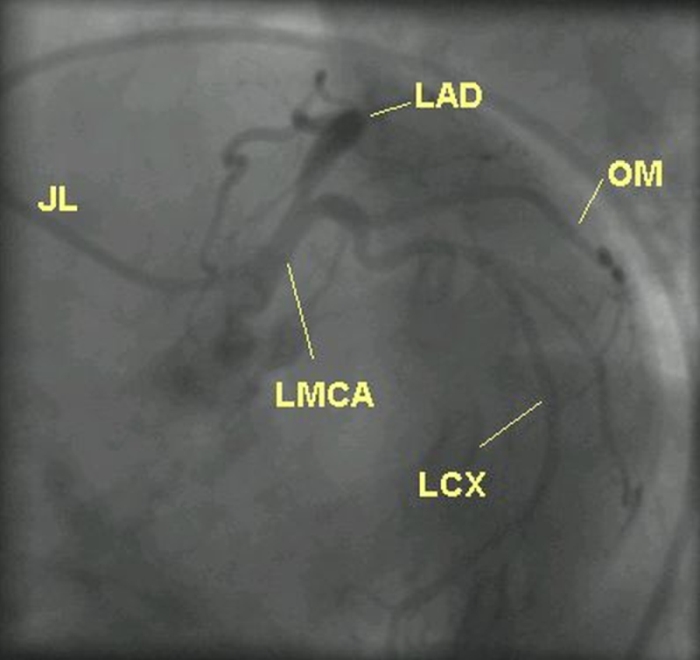
This a left coronary angiogram in LAO caudal view in another case. JL: Judkins left coronary catheter. Difference in the orientation of coronaries could be due to anatomical variations as well as mild changes in angulations used. X-ray penetration will be less in LAO caudal view, especially in obese individuals. In this view mid segment of LAD is foreshortened and hence this view should not be used during angioplasty of mid LAD. But proximal region of LAD is visualised well. Proximal and mid segments of LCX are well seen in this view.
Video of left coronary angiogram in LAO caudal view is shown above, with annotation of branches in a still frame.
RAO caudal view is another common view for the left coronary angiogram. Some operators use this as the first view. Usual angulation is 30-40º to the right. But shallower views may be used sometimes to reduce respiratory movements. Sufficient caudal angulation to separate out the proximal portions of LAD and LCX is used. Proximal and mid portions of LCX and bifurcation of marginal branches are seen. It is a good view for the distal LAD. Diagonal and septal branches may superimpose on the proximal and mid LAD in this view.
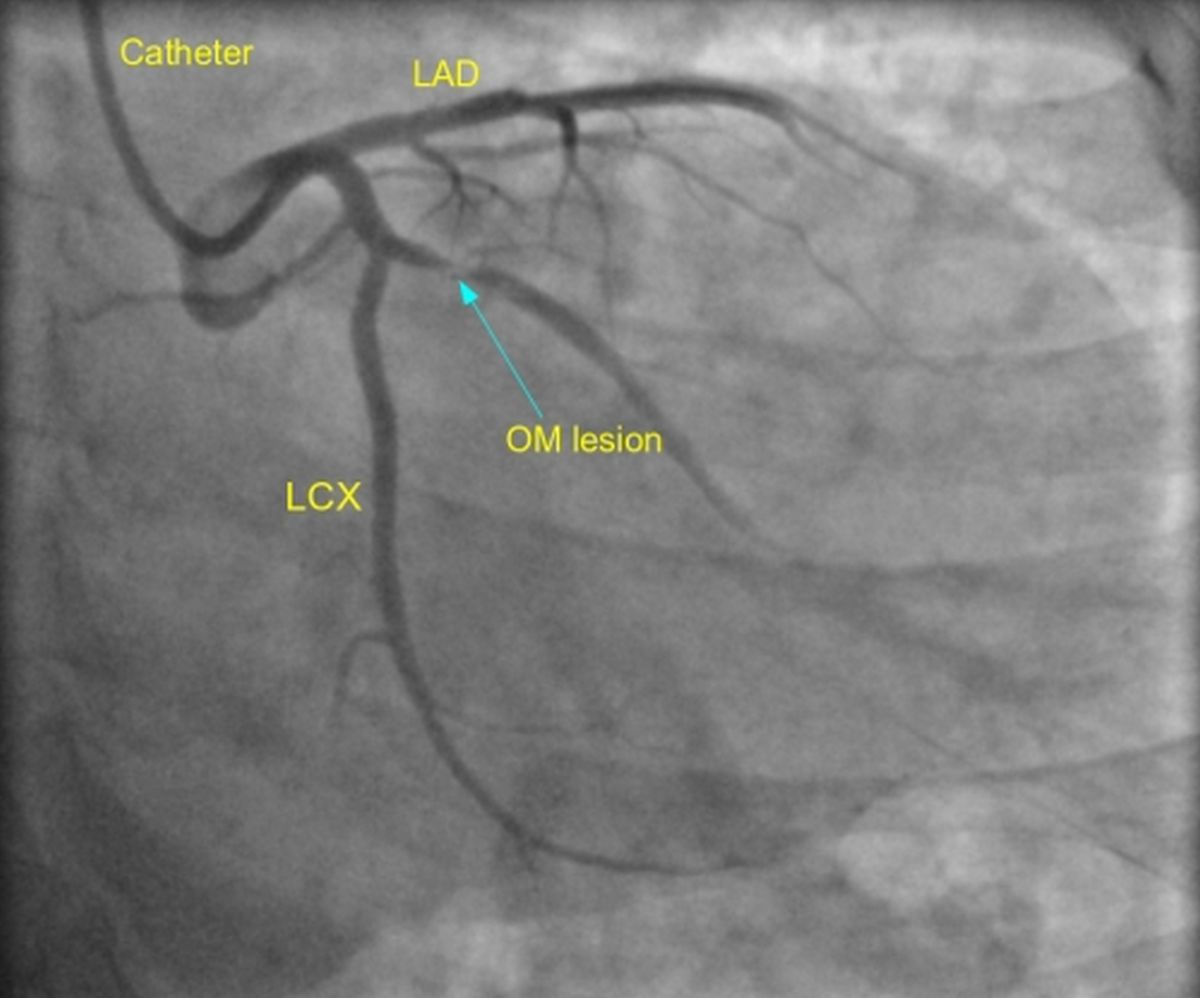
Left coronary angiogram in RAO caudal view showing a tight lesion in the obtuse marginal (OM) branch of the left circumflex (LCX) coronary artery. LAD: left anterior descending coronary artery. The OM lesion is marked by the blue arrow and is seen in the proximal portion of the obtuse marginal, which is a major branch of the left circumflex.
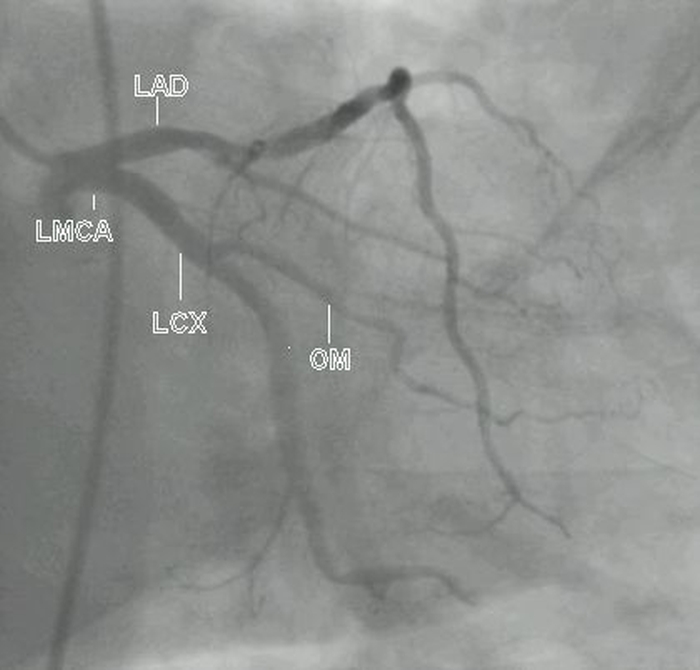
This is a left coronary angiogram in RAO caudal view from another case. Distal LAD is seen well in this case. It can be seen that diagonal and septal branches are overlapping the mid LAD, as mentioned earlier.
AP (PA) cranial view is ideal for most lesions in the proximal and mid LAD. A cranial angulation of 40º shows the diagonal and septal branches in opposite directions, well separated from the LAD.
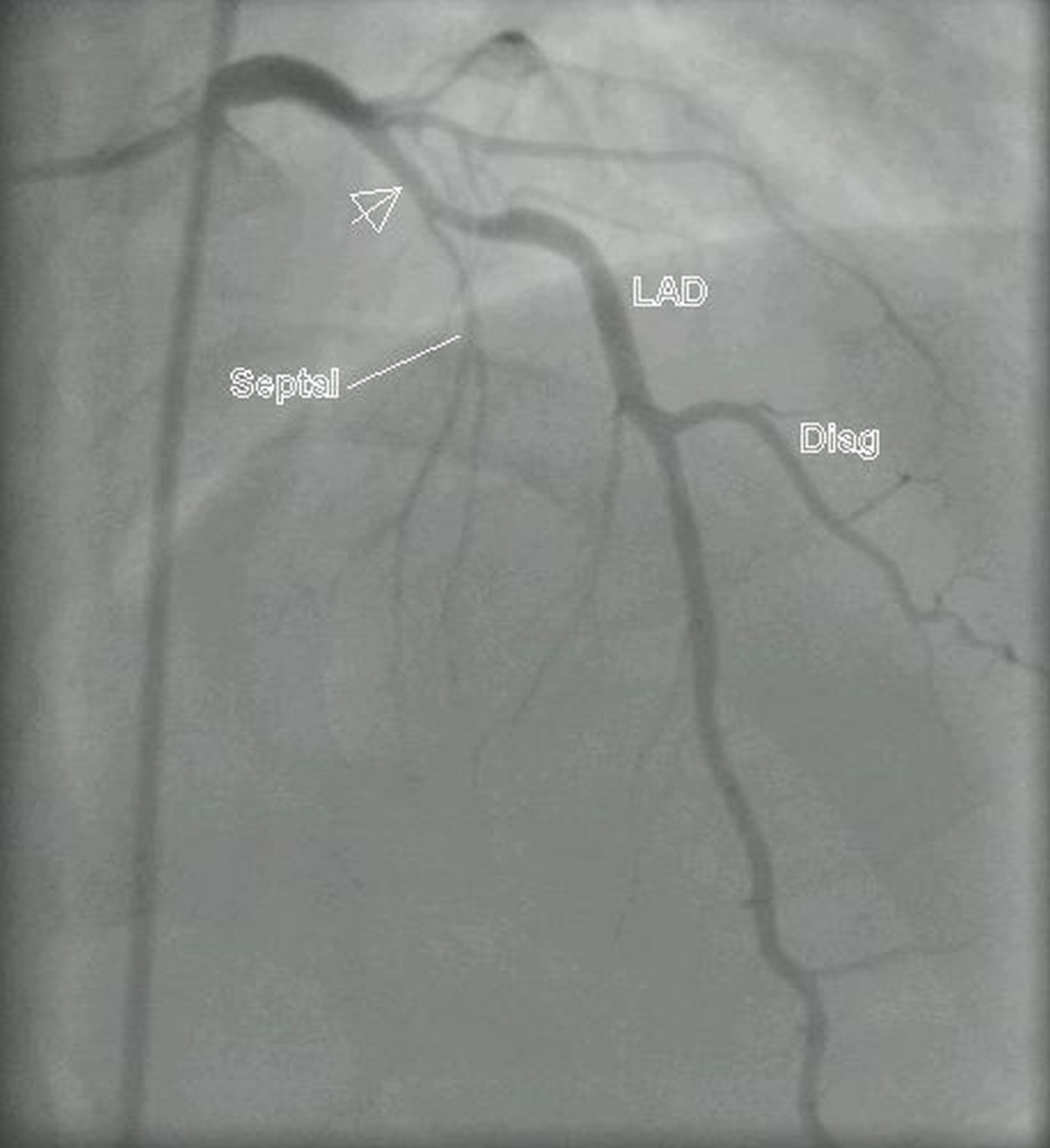
Left coronary angiogram in PA cranial view showing a proximal plaque (arrow) in LAD, in this case a recanalized vessel after anterior wall myocardial infarction. Septal and diagonal (Diag) branches of LAD are also seen. Almost the whole extent of the LAD is seen well. Proximal left circumflex is foreshortened in this view.
Rightward angulation (RAO cranial) is useful in reducing the overlap of proximal LAD by the vertebral spine and the catheter. It may be noted that in both cranial views, the diaphragmatic shadow goes high up into the field.
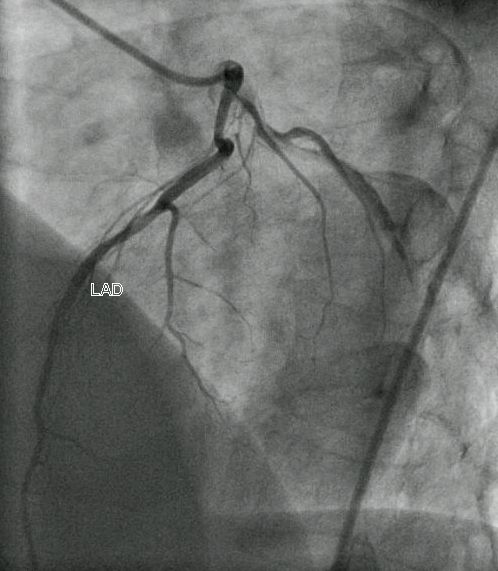
Video of left coronary angiogram in RAO cranial view showing a complex lesion in the LAD. The LAD can be seen wrapping around the apex (type III LAD). Type I LAD will stop short of the apex and type II will reach up to the apex.
LAO cranial view straightens out the proximal and mid LAD. Diagonal branches are seen on the same side as the obtuse marginal branches. Septal perforators are seen to the opposite side [2].
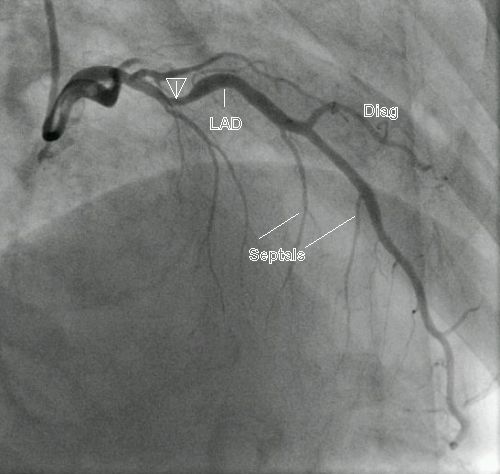
In the left coronary angiogram in LAO cranial view shown above, OM branches of LCX are seen overlapping the spine. Diagonals are seen running down between the spine and the LAD. Septal branches are seen on the opposite side, but almost parallel to the LAD.
Lateral view is seldom used and ideally requires the positioning of the hands above the head to avoid superimposition of patient’s arms. But this requirement is not there when the field of interest is in the distal part of the LAD which is anterior. The same applies to visualisation of the anastomosis between the left internal mammary artery and LAD.
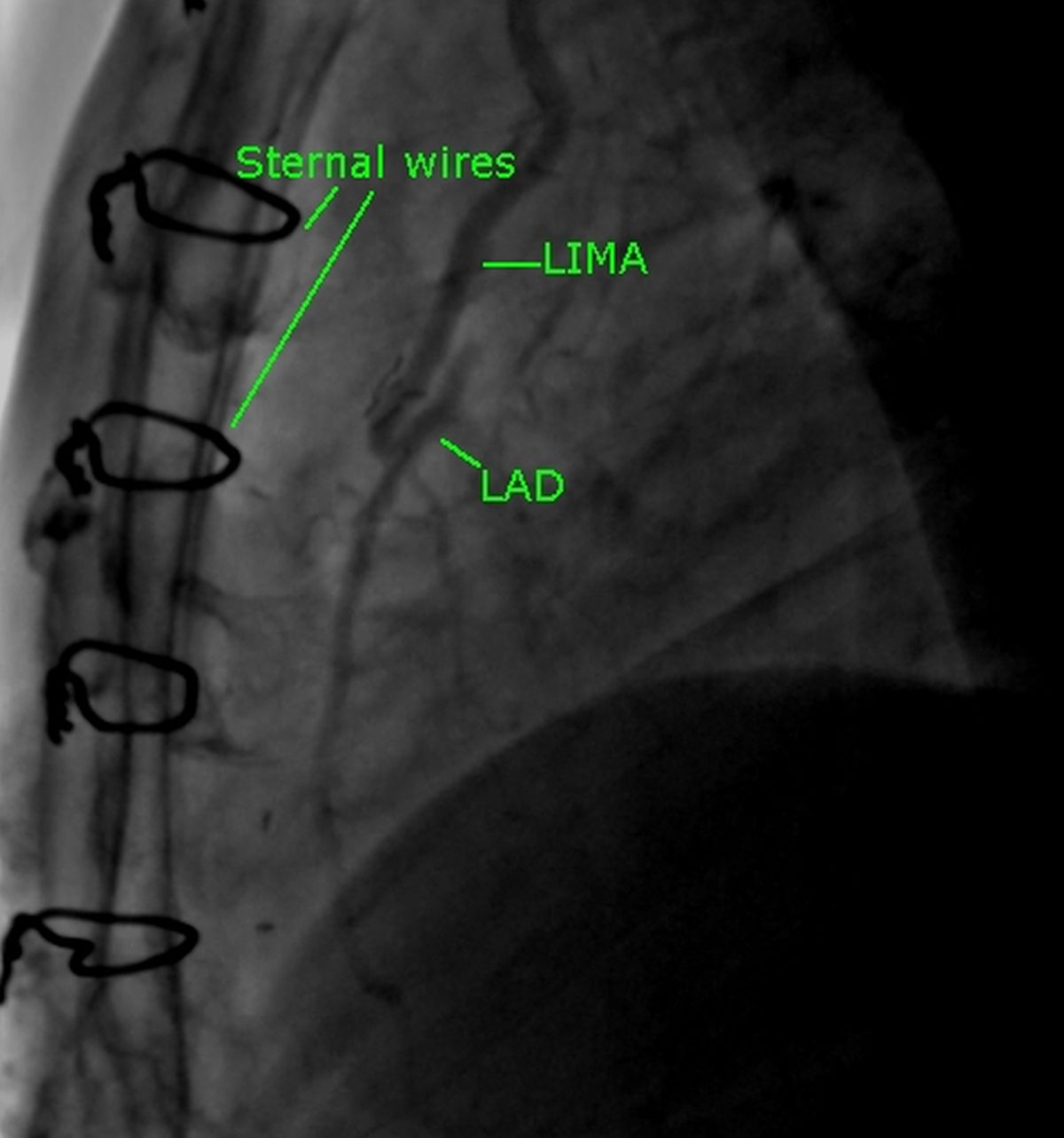
The image above has been darkened a bit by post processing to visualize the LIMA and LAD well. Since it was an injection into the left subclavian artery just near the LIMA ostium, the contrast density was a bit lower than that of a superselective LIMA injection. The sternal wires indicate the post sternotomy status. Distal flow into the LAD is good. Retrograde flow from the anastomotic site into the proximal part of LAD is also seen.
Views for right coronary angiography
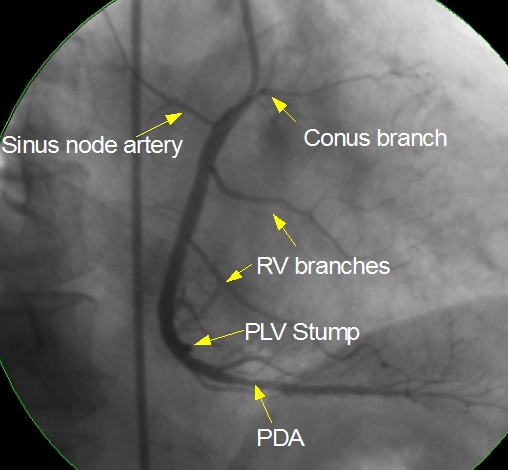
RAO view shows the conus branch and sinus node artery in opposite directions as seen in the image below. Right ventricular branches and posterior descending artery (PDA) are seen well. Multiple septal branches can be seen arising from the PDA. PDA has a mild lesion in the proximal portion. In the angiogram illustrated, the posterior left ventricular branch is occluded and only a stump (PLV stump) is seen. Atrioventricular nodal artery usually originates near the bifurcation of the right coronary artery into PDA and PLV.
Here is another right coronary angiogram in RAO view. Here the septal branches of PDA and PLV branch are well seen.
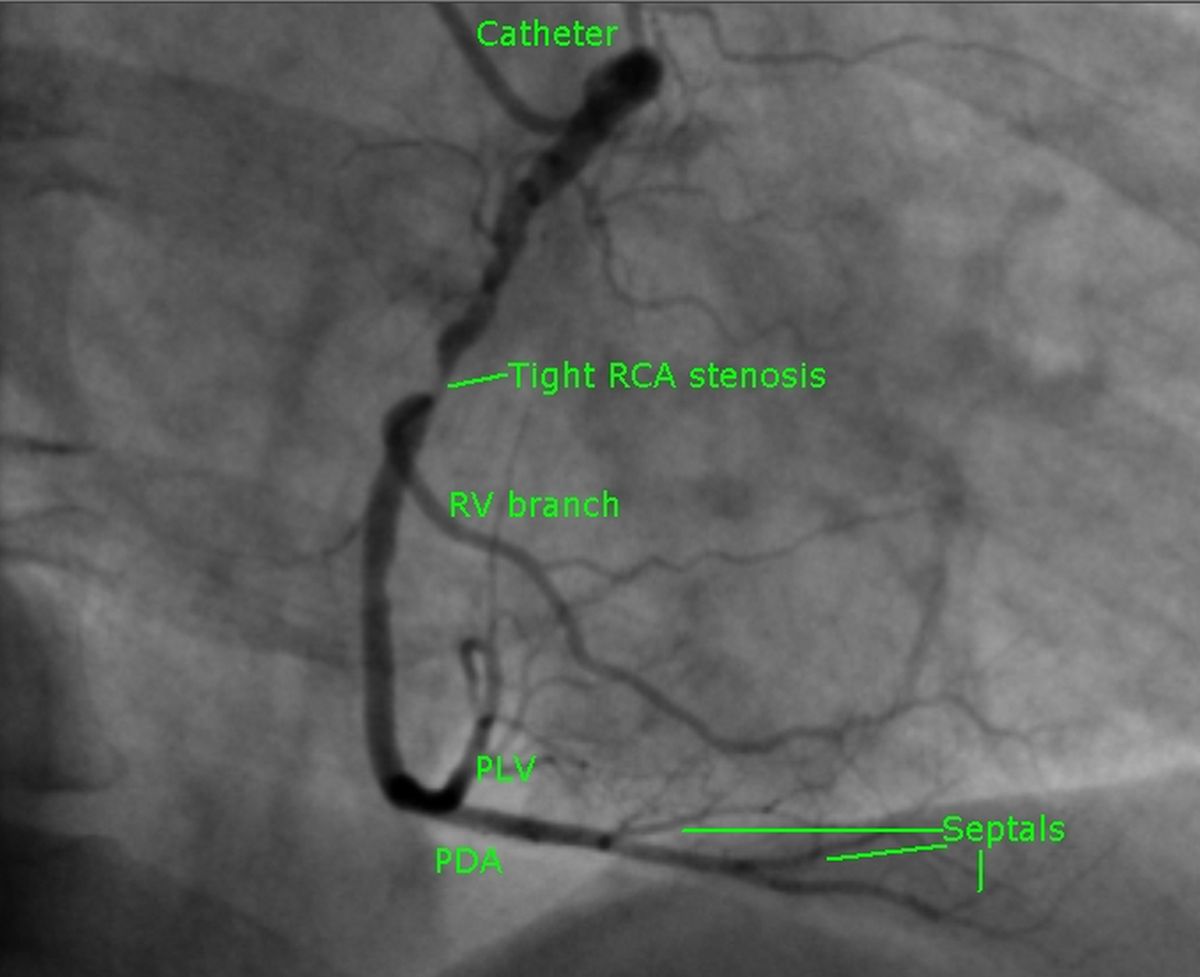
RAO view shows the proximal part of the right coronary artery in a vertical line. RAO view is identified with the spine seen on the right side. Tight stenosis is seen just before the origin of a right ventricular branch.
LAO view usually shows the full length of the right coronary artery in a C shape. Distally the right coronary artery divides into PDA and PLV at the crux cordis. Crux cordis is the junction of the atrioventricular and interventricular grooves posteriorly.
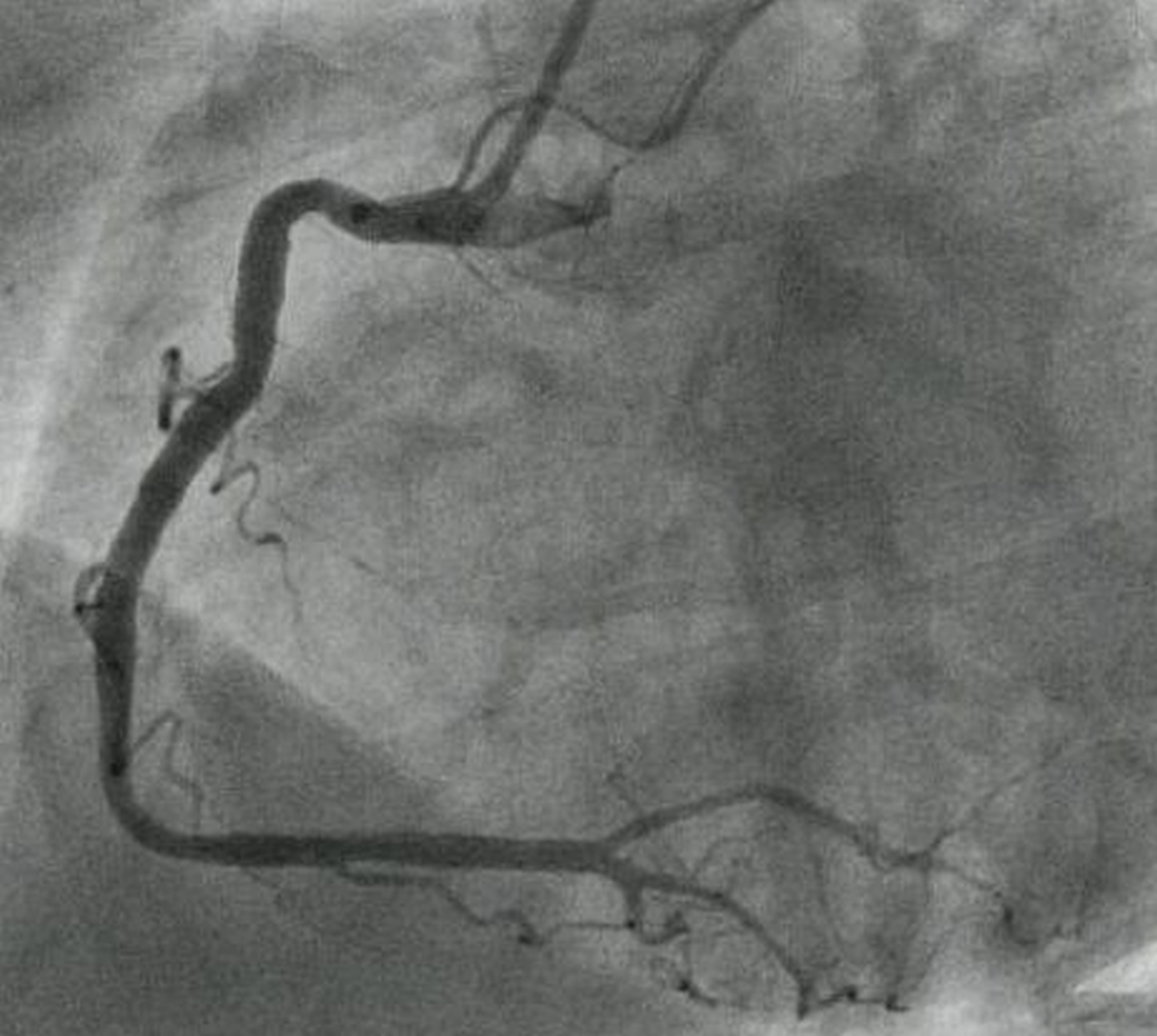
The artery which crosses the crux is defined as the dominant coronary artery. Right coronary dominance is much more common than left dominance. Even when the right coronary artery is dominant, the major portion of left ventricular myocardium is supplied by the left coronary artery.
PA cranial view of right coronary angiogram is shown below. As in other cranial views, diaphragmatic contour can be seen high up in the field.
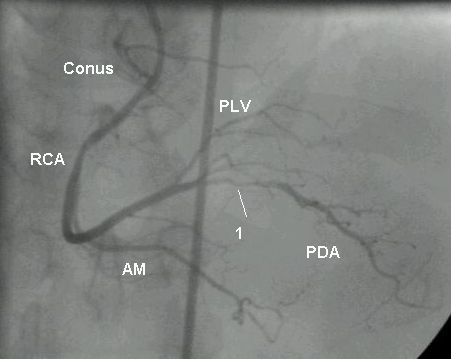
A tight lesion is seen in proximal portion of PDA, marked as 1. PLV: posterior left ventricular branch; AM: acute marginal branch; RCA: right coronary artery. Conus: conus branch of the right coronary artery. Sometimes while cannulating the right coronary artery, the catheter slips into the conus artery. This causes wedging and damping of catheter tip pressure. Prolonged inadvertent injection of contrast into the conus branch can cause ventricular tachycardia or ventricular fibrillation occasionally. A large conus branch crossing the right ventricular outflow tract can cause problem during intra cardiac repair of Tetralogy of Fallot.
LAO cranial view of right coronary angiogram using an Amplatz right catheter is given below.
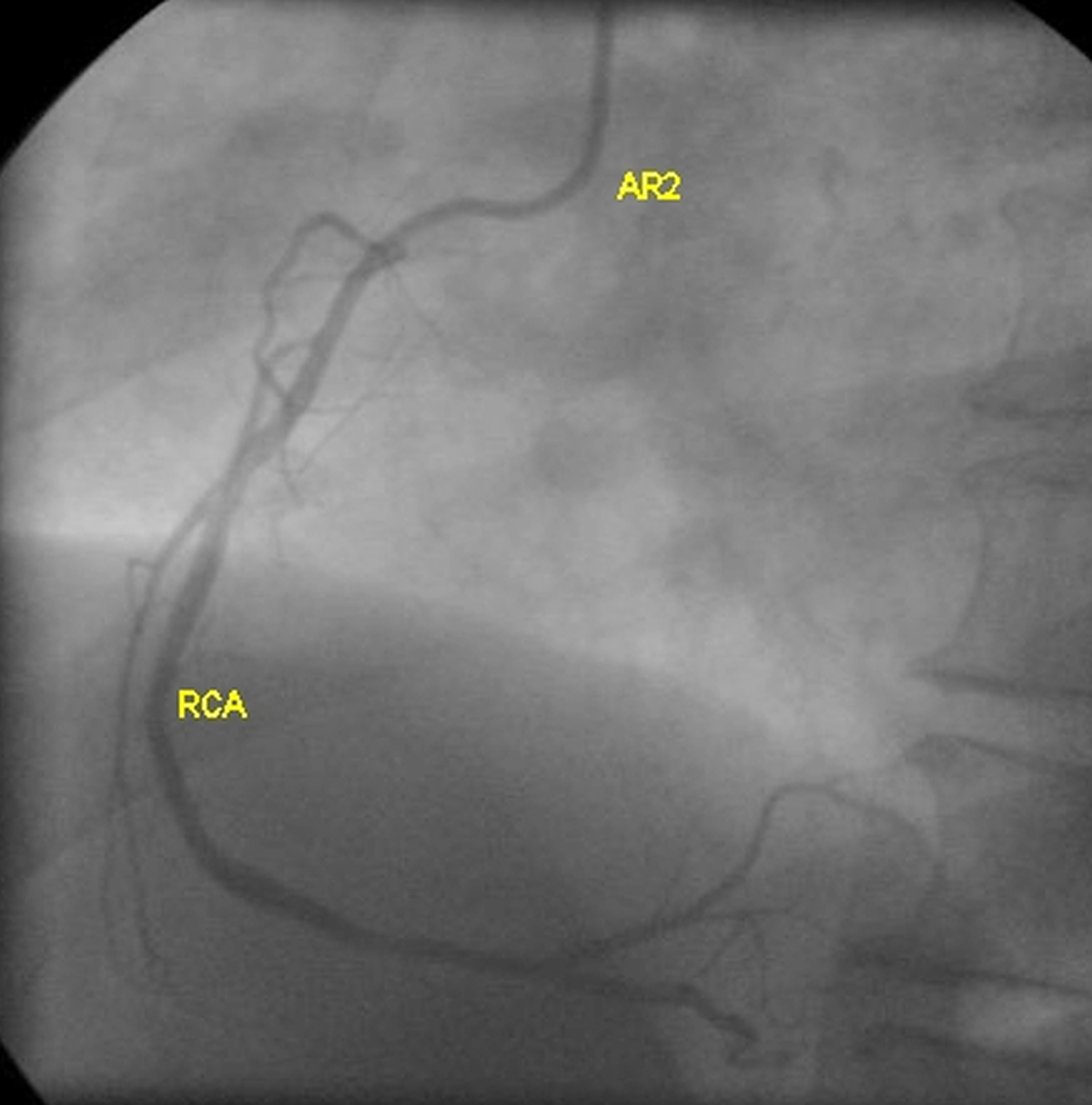
This RCA was difficult to cannulate with Judkins right catheter even after repeated attempts. The angiogram shows only minimal luminal irregularities of the RCA. Right ventricular branches are seen originating from the proximal region and terminal branching of RCA into posterior left ventricular (PLV or PLB) branches and posterior descending coronary artery (PDA).
References
- Di Mario C, Sutaria N. Coronary angiography in the angioplasty era: projections with a meaning. Heart. 2005 Jul;91(7):968-76.
- Aquilina O, Grech V, Felice H, Debono J, Fenech A. Normal adult coronary angiography. Images Paediatr Cardiol. 2006 Apr;8(2):1-16.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal