ECG and CXR in ASD
ECG and CXR in ASD
ECG in atrial septal defect
Atrial fibrillation may be seen in adults. Atrial flutter can occur in ASD, even after repair. Inverted P waves seen in inferior leads indicate low atrial rhythm (also known as coronary sinus rhythm) in sinus venosus atrial septal defect. This is due to defective sinus node as the septal defect is in the region of the sinoatrial node. Classical QRS pattern in ASD is the rSR’ in V1 suggestive incomplete right bundle branch block. This pattern in ASD is due to right ventricular volume overload. QRS axis is usually rightward, more so when there is severe pulmonary hypertension. Left axis deviation is feature of ostium primum ASD. First degree AV block may be noted in both primum and secundum ASD. Familial ASD with first degree AV block has been reported in secundum ASD. This type of familial ASD has an autosomal dominant inheritance pattern. There is also a higher incidence of sudden cardiac death in this group.
Right atrial overload is often seen in ASD. Left atrial overload and left ventricular volume overload patterns can occur if there is severe mitral regurgitation associated with ostium primum ASD.
Notching of R wave near the apex in inferior leads has been called crochetage sign in ASD. The crochetage sign has a sensitivity of about 73% and specificity of 92%, if the sign is present in all the three inferior leads. Early disappearance of the crochetage sign after surgical correction of atrial septal defect was found in 35% of cases even when the incomplete right bundle branch block (IRBBB) pattern was persisting.
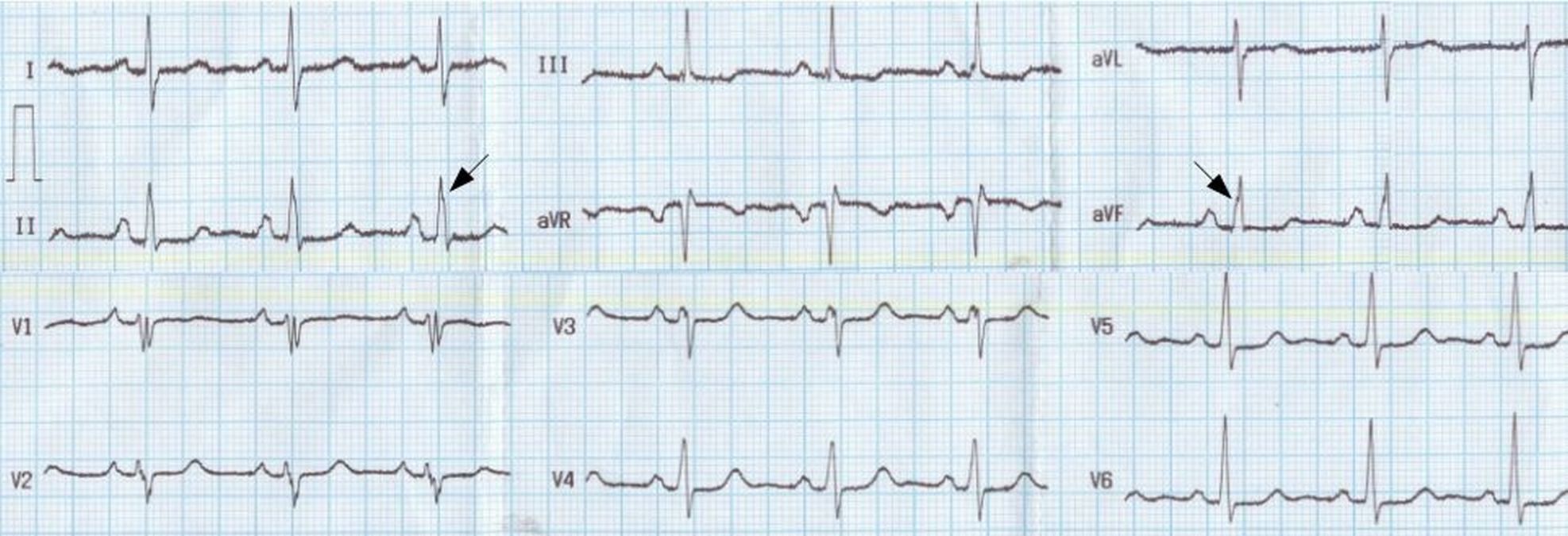
Crochetage sign in ASD, manifest as notching of R wave near the apex in inferior leads (arrows). Sharp P waves in V1 and 3 mm tall P waves in lead II suggest right atrial overload. rSr’S’ pattern in V1 is suggestive of right ventricular volume overload.
When there is severe pulmonary hypertension in ASD, right ventricular hypertrophy and strain patterns are manifest in the ECG. The secondary R wave in V1 is tall and ST segment depression with T wave inversion are found in the anterior and inferior leads.
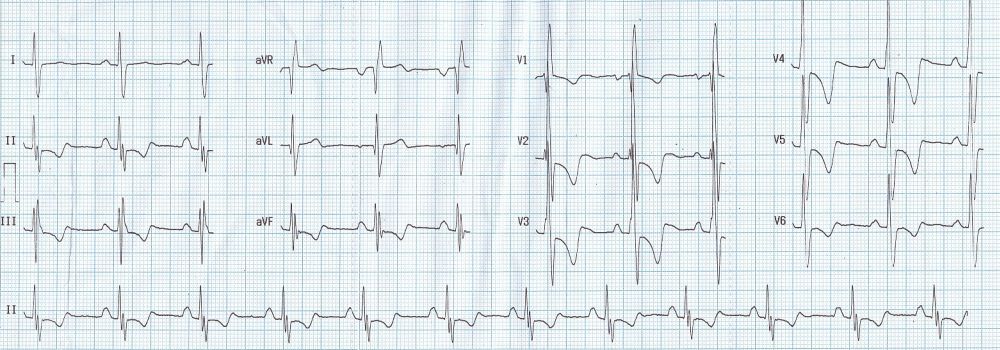
ECG in ASD with severe pulmonary hypertension: Tall R’ in V1, ST depression in inferior leads and V2-V5, and T inversion in inferior leads and V1-V6 are seen.
Chest X-ray in atrial septal defect
The classical finding of chest X-ray (CXR) in atrial septal defect is pulmonary plethora, due to increased vascularity. This is seen when there is a large left to right shunt. More than five end on vessels, seen as circular shadows, are also often noted. The main pulmonary artery is prominent, along with right and left pulmonary arteries (Figure 10.8). The pulsations of prominent hilar pulmonary arteries on fluoroscopy has been called hilar dance. Right atrial enlargement occurs later on, manifest as a shift of the right border towards the right from the midline. In ASD with large left to right shunt, the cardiac apex is of the right ventricular type (upturned). When there is associated severe mitral regurgitation, a down and out left ventricular apex may be noted.
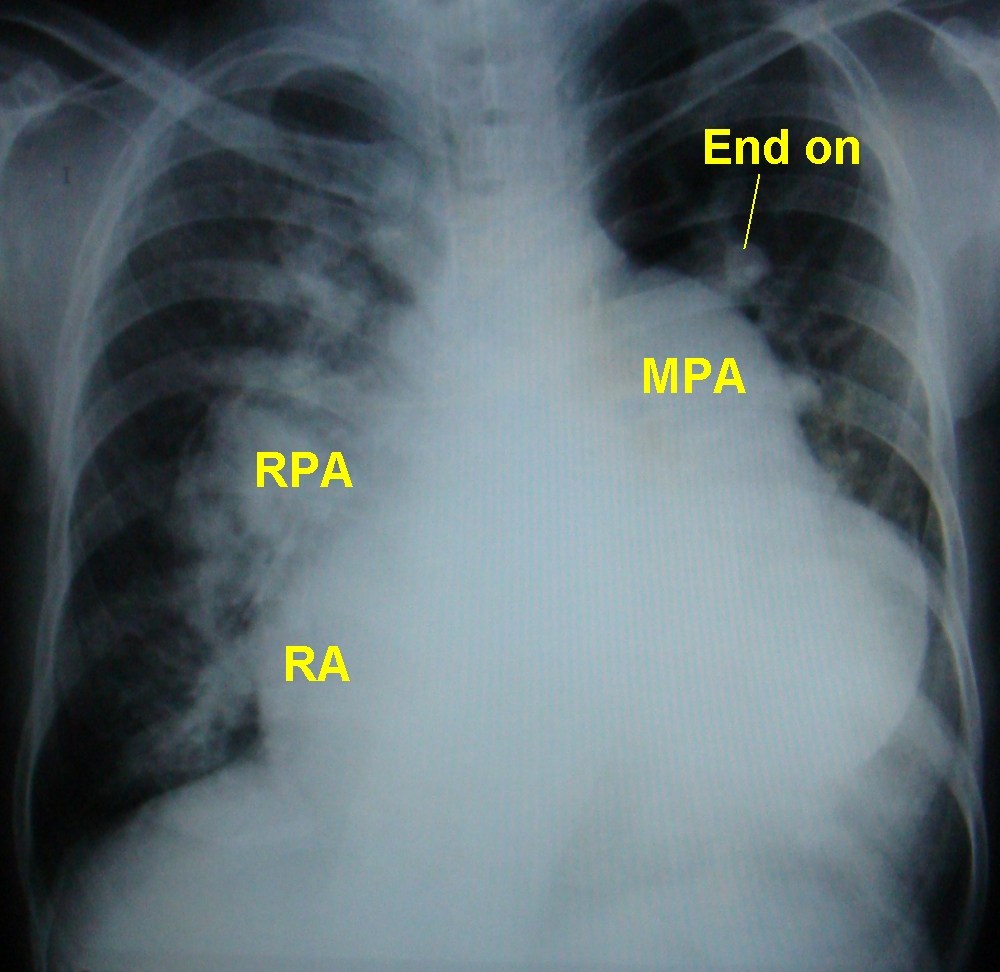
Chest X-ray in atrial septal defect with pulmonary hypertension: Prominent main pulmonary artery (MPA) and right pulmonary artery (RPA) are seen. Left pulmonary artery shadow is retrocardiac, descending from the MPA segment. Right atrial enlargement (RA) is visible. Cardiac apex is upturned suggestive of right ventricular apex. End on vessels are also seen.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal