ECG and CXR in ventricular septal defect
ECG and CXR in ventricular septal defect
ECG in ventricular septal defect
ECG is normal in a small ventricular septal defect. Large VSD with large left to right shunt will have left ventricular volume overload with small q, tall R and upright T waves in lateral leads. Large VSD progresses to biventricular overload when there is hyperdynamic pulmonary hypertension. The ECG pattern of biventricular hypertrophy is called Katz – Wachtel phenomenon with tall biphasic (R=S) QRS complexes with amplitude over 50 mm in mid precordial leads. This pattern is usually seen in children. Since the QRS amplitude is high it often overshoots the margin of the ECG graph as seen in lead V4 in this case. It may be necessary to take ECG in half standardization (5 mm to a millivolt instead of 10 mm to a millivolt) to capture the full QRS complex without overlapping with other leads in simultaneous multichannel recordings. Standard single channel ECG paper has a height of 50 mm for the graph. Large anterior electrocardiographic forces are due to the hypertrophied right ventricle and late posterior forces due to the hypertrophied left ventricle.
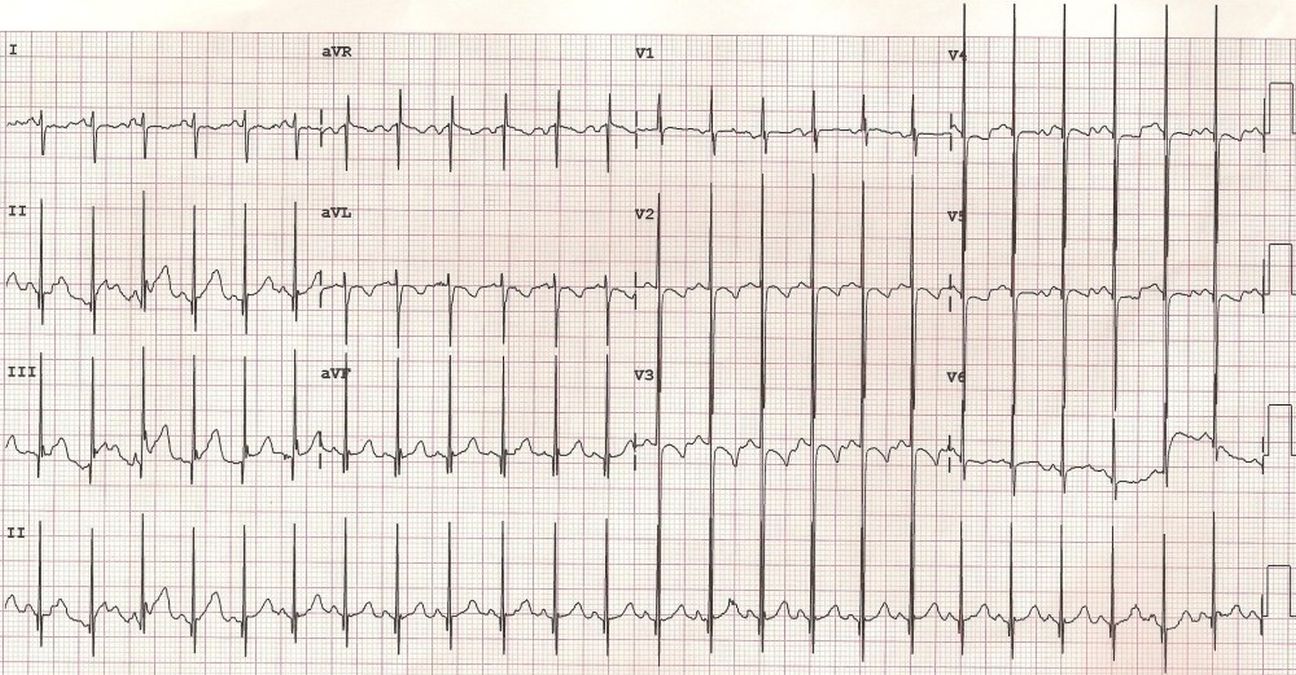
Tall biphasic QRS complexes in mid precordial leads suggestive of Katz-Wachtel phenomenon in VSD with large left to right shunt.
AV canal VSD (inlet VSD, endocardial cushion defect) is associated with left axis deviation in the ECG. Complete heart block, both transient and permanent can occur after surgical repair of ventricular septal defect as well as after device closure. This is because of the proximity of the defect to the conduction system.
X-ray chest (CXR) in ventricular septal defect
Chest X-ray is normal in a small ventricular septal defect. Large ventricular septal defect will have left ventricular type of cardiomegaly and pulmonary congestion in infancy before the development of pulmonary hypertension. Pulmonary hypertension manifests on CXR as prominent main pulmonary artery segment and prominent right descending pulmonary artery. Close scrutiny may show the dilated left pulmonary artery within the cardiac silhouette. When severe pulmonary hypertension occurs, cardiac size decreases due to decrease in the pulmonary blood flow. But pulmonary arteries become more prominent. Initially pulmonary vascular markings are prominent and seen up to the periphery of the lung fields with large left to right shunt. When vasoreactive pulmonary hypertension sets in there is peripheral pruning with decrease in vascular markings in the periphery of the lung fields.
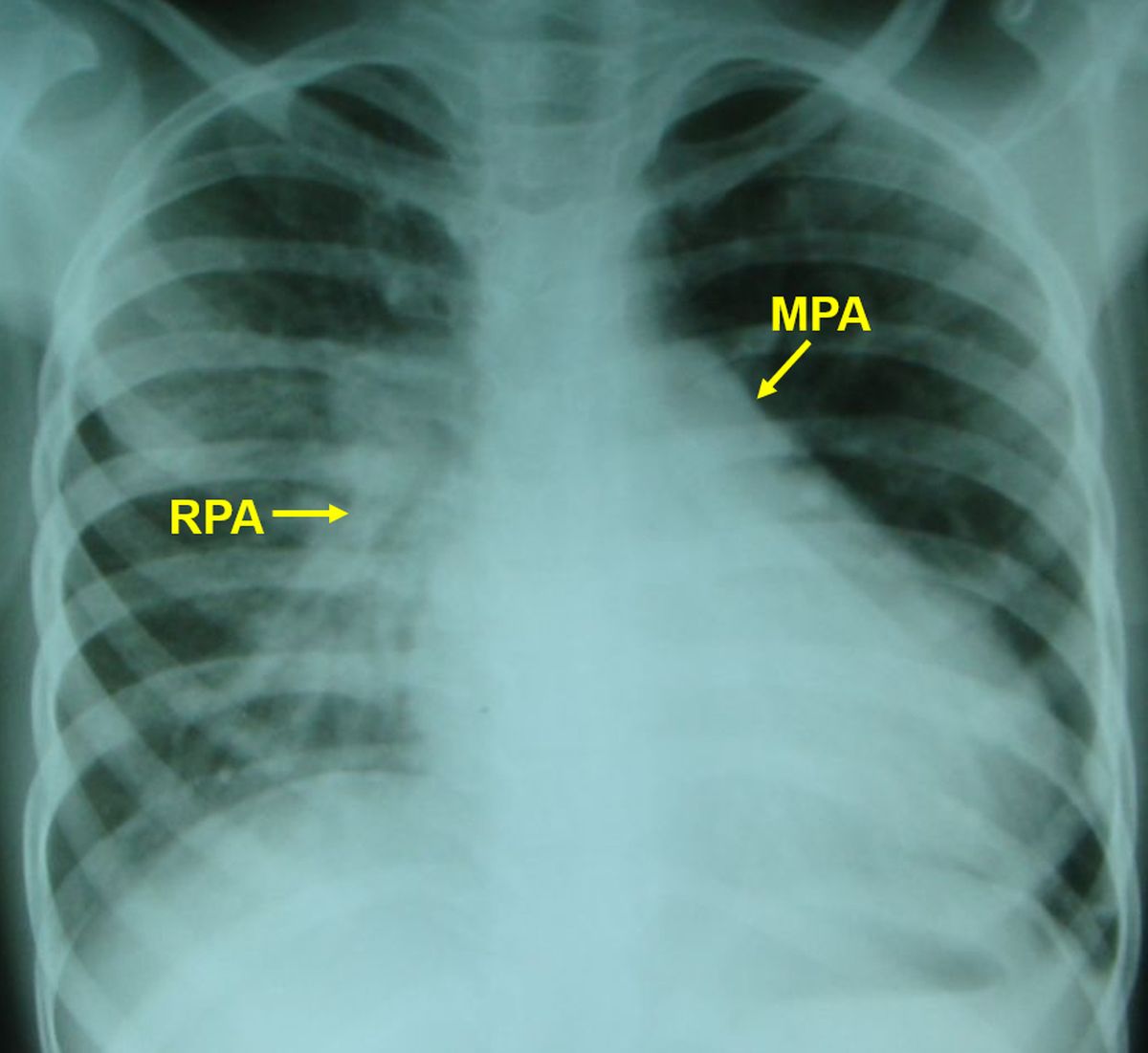
X-Ray chest PA View of a child with ventricular septal defect and left to right shunt and hyperdynamic pulmonary hypertension. There is cardiomegaly, prominent main pulmonary artery segment and right pulmonary artery. Enlarged left pulmonary artery shadow is seen below the left cardiac border, within the cardiac silhouette. The enhanced vascular markings are visible on the right side whereas it is obscured by the cardiac shadow on the left side. This child ideally needs cardiac catheterization for evaluation of shunt and pulmonary vascular resistance and its reversibility to decide on surgical option.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal