ECG Quiz 62
ECG Quiz 62
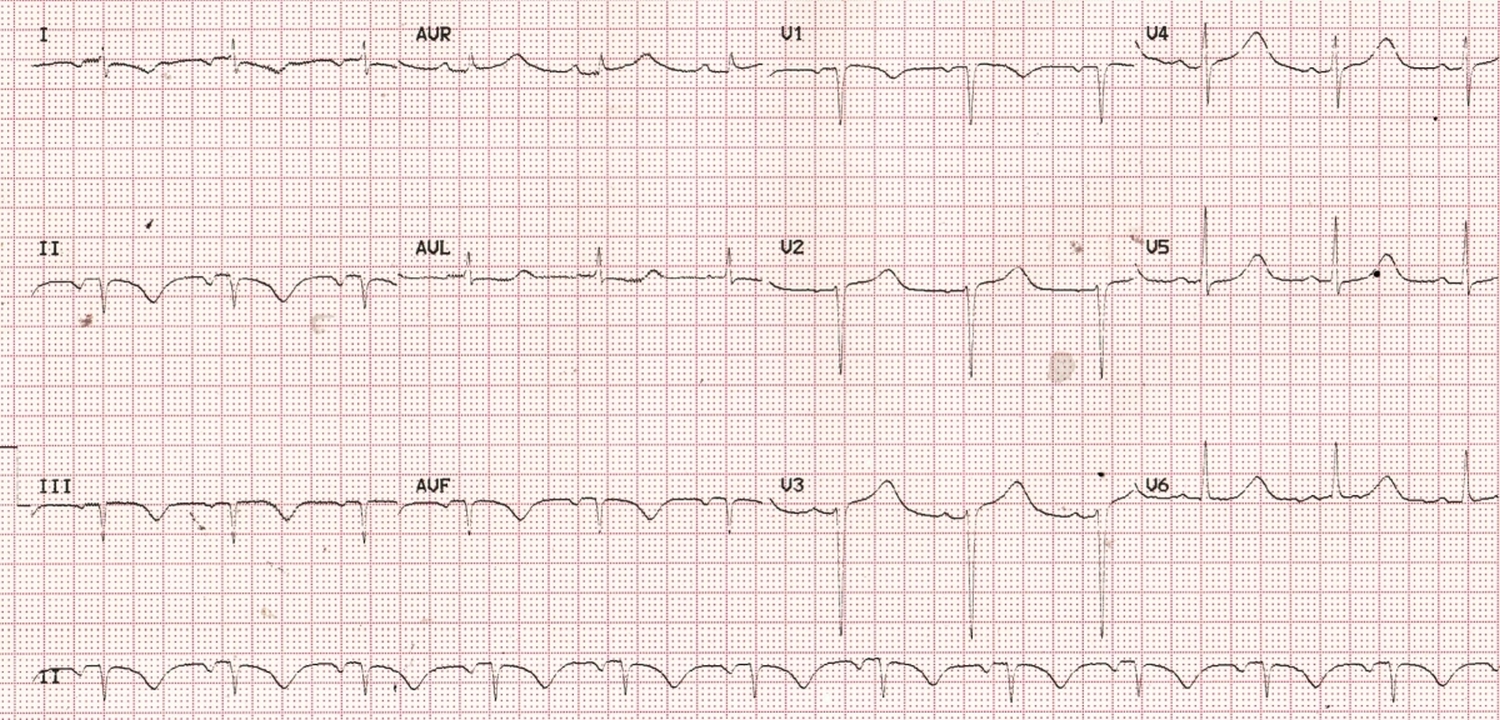
At one look it appears like an evolved inferior wall myocardial infarction. But on close scrutiny, the inverted P waves in lead I and inferior leads catch your attention. PR interval is 200 milliseconds. Some would think that this could be a rhythm other than sinus rhythm, originating from the lower left portion of the atrium. In left atrial rhythm one would expect P inversion in lead I, V6 and inferior leads. But that will not change the QRS pattern or T waves. Here we have QS complexes in inferior leads with T wave inversion. Down sloping ST with T wave inversion is seen in lead I.
QT interval is 480 ms with RR interval 0.88 seconds. Corrected QT interval calculate by Bazett’s formula, is 511 milliseconds, which is definitely quite prolonged. Hypokalemia, hypomagnesemia and hypocalcemia have to be checked for. One would have expected lower amplitude of T waves in typical hypokalemia.
Bazett’s formula: QTc = Observed QT/square root of RR interval in seconds [1].
Now coming back to the initial observations, what looks like an inferior wall infarction with a rhythm other than sinus rhythm with abnormal P wave axis can occur when the right arm and left leg leads are reversed while recording the ECG [1]. Simplest way to check for lead errors is to take a repeat ECG under direct supervision and compare the tracings. In this case, inferior wall infarction pattern and abnormal P wave axis reverted in the repeat ECG. Sometimes one may have a doubt whether it was a transient supraventricular rhythm abnormality. But then, QRS abnormalities reverting back to normal rules out that possibility.
Lead reversals are one of the common technical errors during ECG recording, commonest being right arm left arm lead reversal. Right arm – left arm lead reversal is often called technical dextrocardia as standard leads recorded in that situation resembles that in dextrocardia. Chest leads will not be altered in that case and clinches the technical error.
Returning to the current ECG, the technical error will not explain the prolongation of QT interval, for which usual causes will have to be sought and found.
Most of the modern electrocardiographs with analytic programs built in usually recognize right arm – left arm lead reversal and give a warning note. Some mention that the interpretation given is presuming a normal lead placement. Other lead reversals are difficult to diagnose both for the algorithm and for the interpreting physician.
Artificial neural networks have been used for recognition of electrocardiographic lead reversal [3]. 11,009 ECGs recorded using computerized electrocardiographs in an emergency department were used for the study. Right arm – left arm lead reversals where then computationally created for each ECG. Neural networks were then trained to detect ECG with right arm – left arm lead reversal. The neural networks performed better than rule based criteria regardless of whether P waves were present or absent. Neural networks had a sensitivity of 99.1% when P waves were present and 94.5% when P waves were absent. Corresponding sensitivities for the best criteria were 93.9% and 39.3% respectively. Both neural networks and rule-based criteria had very high specificity of 99.87% to 100%. It is mentioned that neural networks along with an algorithm for detection of right arm – right foot lead reversal would recognize about three fourths of lead reversals seen in clinical practice [4]. These technologies should be used as guide to alert us to frequently overlooked lead attachment errors, for avoiding errors in electrocardiographic diagnosis.
References
- Bazett HC. An analysis of the time-relations of electrocardiograms. Heart. 1920;7: 353–370.
- Peberdy MA, Ornato JP. Recognition of electrocardiographic lead misplacements. Am J Emerg Med. 1993 Jul;11(4):403-5.
- Hedén B, Ohlsson M, Edenbrandt L, Rittner R, Pahlm O, Peterson C. Artificial neural networks for recognition of electrocardiographic lead reversal. Am J Cardiol. 1995 May 1;75(14):929-33.
- Hedén B, Ohlsson M, Holst H, Mjöman M, Rittner R, Pahlm O, Peterson C, Edenbrandt L. Detection of frequently overlooked electrocardiographic lead reversals using artificial neural networks. Am J Cardiol. 1996 Sep 1;78(5):600-4.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
SR, rate of aroud 70 bpm, regular, Pwave: inverted in I,II,III,aVF andupright in aVR,
PR:120msec, QRSd: 60msec,
inverted QRS in II,III,aVF and upright in aVR
suggestive of limb lead reversal
here Rt arm and Lt foot electrodes are interchanged
other wise normal EKG
Good observations
Rt UL and Lt LL leads interchanged, QT prolonged
Excellent observations
Prolonged QT interval, clear upright U wave after inverted T waves — advice to check K and Mg
Likely Hypokaelemia