Kawasaki disease and coronary involvement
Kawasaki disease and coronary involvement
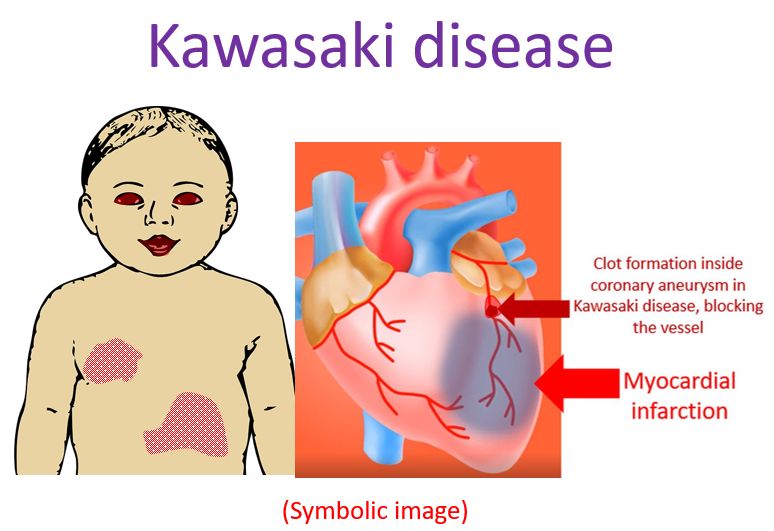
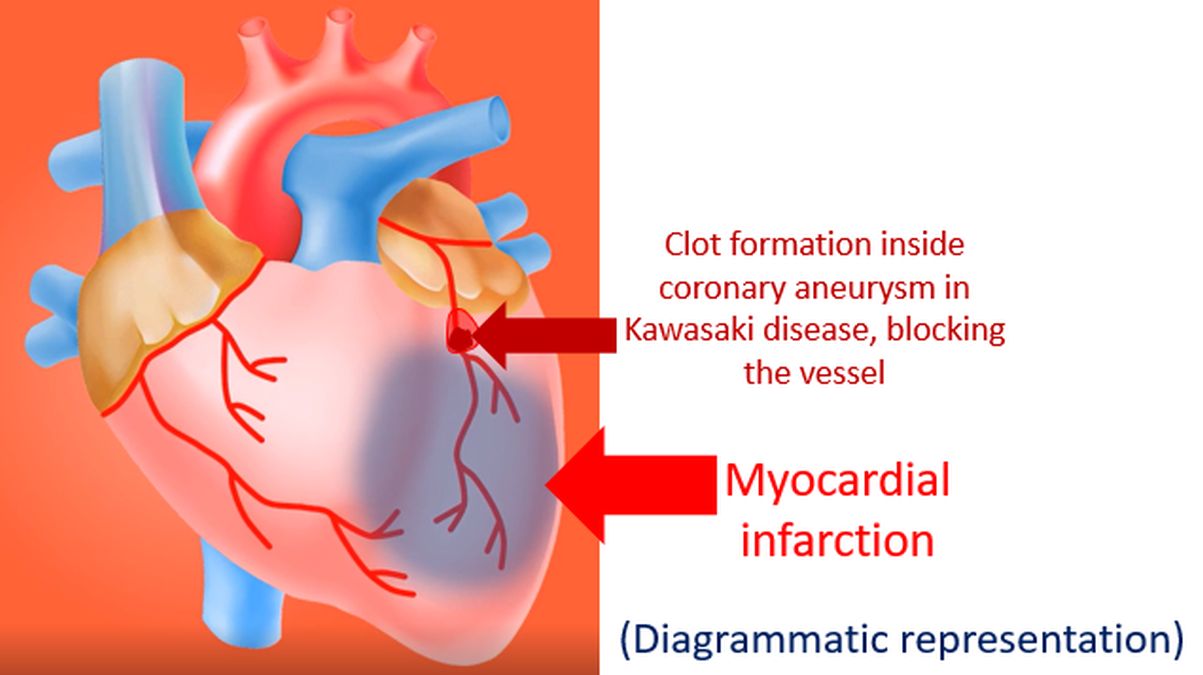
Kawasaki disease, also known as mucocutaneous lymph node syndrome is an acute febrile illness in children, usually less than 5 years of age. It was first described by Tomisaku Kawasaki in Japan in 1967. Now Kawasaki disease is known to occur globally. Important features include fever, rash, swelling of hands and feet, lymphadenopathy and involvement of eyes, lips, throat and coronary arteries. Most important sequelae of Kawasaki disease is coronary dilatation and aneurysm formation.
As per data available on the US Centres for Disease Control and Prevention website, incidence of Kawasaki disease ranges from 9 to 20 per 100,000 children below the age of 5 years. 5440 hospitalizations with Kawasaki disease were reported in children under 18 years of age in the United States in 2016. Of these, 3935 children were under the age of 5 years. This corresponded to a hospitalization rate of 19.8 per 100,000 children in that age group [1].
Z- score has been used for classification of coronary aneurysms in Kawasaki disease. American Heart Association classification of coronary artery aneurysms based on Z-score is as follows [2]: 1. No involvement with Z score less than 2 always. 2. Dilatation only with Z scores from 2 to less than 2.5 or a decrease in Z score of 1 or more during follow up if it was less than 2 initially. 3. Small aneurysm with Z score of more than 2.5, but less than 5. 4. Medium aneurysm with Z score 5 or more, but less than 10 and absolute dimension less than 8 mm. 5. Large or giant aneurysm with Z score 10 or more or absolute dimension 8 mm or more. The decrease in dimension in Class 2 over time means that though the diameter was in normal range initially, it was actually dilated for that person and decreases in size over time.
Factors which favour regression of coronary aneurysms in Kawasaki disease [3]:
- Age less than one year at onset of Kawasaki disease
- Smaller aneurysms have a greater chance of regression
- Distal aneurysms are more likely to regress
- Fusiform aneurysms regress more often than saccular aneurysms
Overall about half to two thirds of coronary aneurysms in Kawasaki disease have been shown to regress on angiography within one to two years of onset of illness. In contrast to coronary aneurysms which can regress with time, stenotic lesions are more likely to progress as they are due to intense myointimal proliferation. Progression of stenotic lesions are more likely in those with giant aneurysms. Worst prognosis is for those with giant aneurysms of 8 millimeters or more diameter [4]. Though echocardiography is the most commonly used investigation for aneurysms in Kawasaki disease and coronary angiography the gold standard, multi detector computed tomography (MDCT) is a useful non invasive modality for long term follow up [5].
Ulinastatin, a urinary trypsin inhibitor and a suppressor of neutrophils, has been shown to reduce the rates of coronary lesions in patients with Kawasaki disease (3% versus 7%; P=0.01). Higher plasma levels of neutrophil elastase and markedly activated neutrophils have been associated with poor response to intravenous immunoglobulin (IVIG) and coronary artery lesions in Kawasaki disease. The retrospective study could identify 369 patients who were treated with a combination of ulinastatin, intravenous immunoglobulin and aspirin. 1178 patients who were treated with IVIG and aspirin served as the control group [6].
Long term data on follow up of patients with Kawasaki disease and giant coronary aneurysms is available. 76 patients with giant coronary aneurysms from an institutional data base since 1972 were identified. The average age at onset was about 3 years and the median follow up was about two decades. Seven of them died and one underwent cardiac transplantation over the follow up period. The survival rates calculated were 95% at ten years and 88% at thirty years. About two thirds of them had undergone surgical or catheter based interventions to alleviate coronary ischemia. The authors called for further research on the role of coronary interventions in those with coronary aneurysms following Kawasaki disease [7].
References
- Kawasaki Disease. Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/kawasaki/about.html. Accessed on 4 July 2022.
- McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, Baker AL, Jackson MA, Takahashi M, Shah PB, Kobayashi T, Wu MH, Saji TT, Pahl E; American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Cardiovascular Surgery and Anesthesia; and Council on Epidemiology and Prevention. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation. 2017 Apr 25;135(17):e927-e999.
- Takahashi M, Mason W, Lewis AB. Regression of coronary aneurysms in patients with Kawasaki syndrome. Circulation. 1987;75:387-394.
- Fujiwara T, Fujiwara H, Hamashima Y. Size of coronary aneurysm as a determinant factor of the prognosis in Kawasaki disease: clinicopathologic study of coronary aneurysms. Prog Clin Biol Res. 1987;250:519-520.
- Khositseth A, Siripornpitak S, Pornkul R, Wanitkun S. Case report: Giant coronary aneurysm caused by Kawasaki disease: follow-up with echocardiography and multidetector CT angiography. Br J Radiol. 2008 Apr;81(964):e106-9. doi: 10.1259/bjr/23978674. PMID: 18344266.
- Kanai T, Ishiwata T, Kobayashi T, Sato H, Takizawa M, Kawamura Y, Tsujimoto H, Nakatani K, Ishibashi N, Nishiyama M, Hatai Y, Asano Y, Kobayashi T, Takeshita S, Nonoyama S. Ulinastatin, a urinary trypsin inhibitor, for the initial treatment of patients with Kawasaki disease: a retrospective study. Circulation. 2011 Dec 20;124(25):2822-8.
- Kenji Suda, Motofumi Iemura, Hiroshi Nishiono, Yozo Teramachi, Yusuke Koteda, Shintaro Kishimoto, Yoshiyuki Kudo, Shinichi Itoh, Haruka Ishii, Takafumi Ueno, Tadashi Tashiro, Masakiyo Nobuyoshi, Hirohisa Kato, Toyojiro Matsuishi. Long-term prognosis of patients with Kawasaki disease complicated by giant coronary aneurysms: a single-institution experience. Circulation. 2011 May 3;123(17):1836-42.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal