Kussmaul’s sign in chronic constrictive pericarditis
Kussmaul’s sign in chronic constrictive pericarditis
Kussmaul’s sign in chronic constrictive pericarditis: It was way back in 1873 that Kussmaul reported that in two patients with constrictive pericarditis, the expected inspiratory collapse of neck veins was replaced by increased inspiratory distension [1]. Since then it has become widely accepted as a sign of constrictive pericarditis (Kussmaul’s sign). But it is not specific for constrictive pericarditis and can occur in other conditions like congestive heart failure, restrictive cardiomyopathy, right ventricular infarction and acute cor pulmonale. But it is not a feature of pericardial tamponade and is useful in distinguishing tamponade from pericardial constriction.
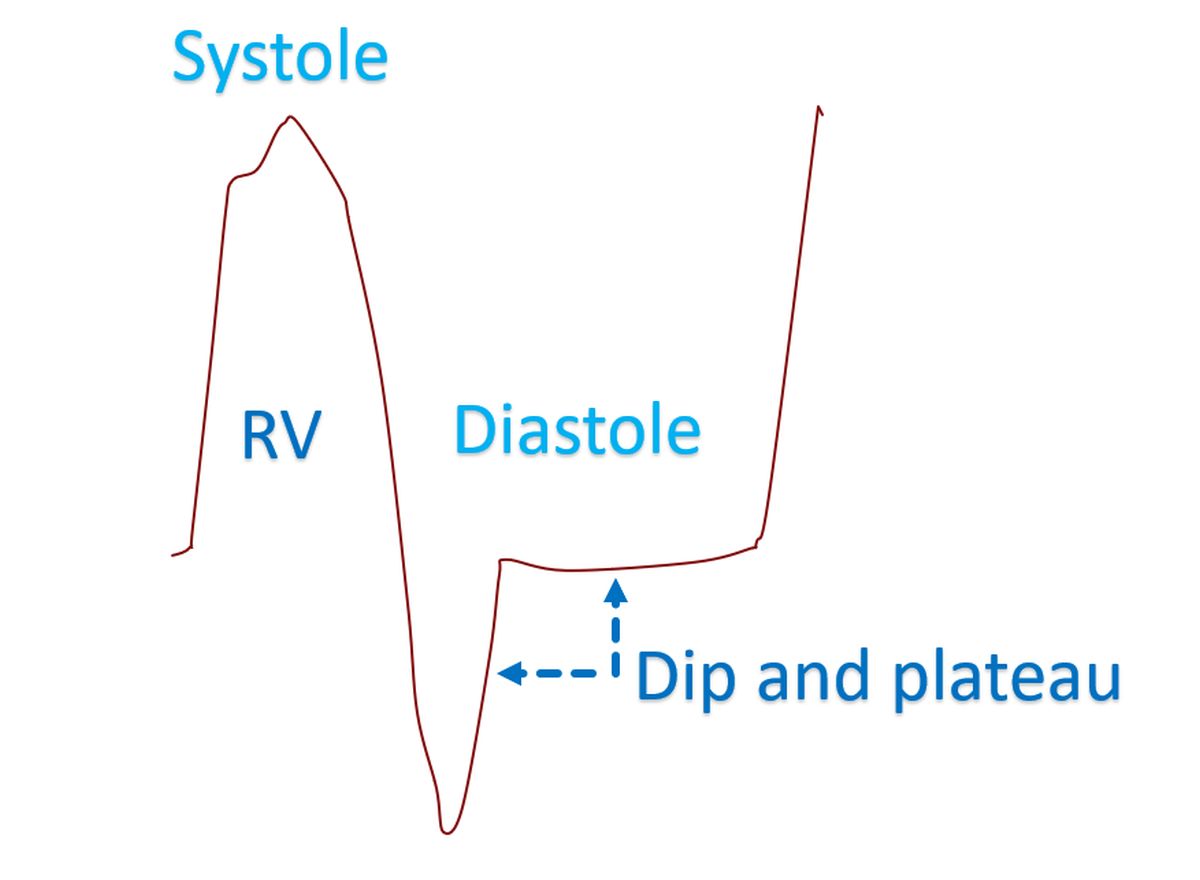
Explanation for the Kussmaul’s sign in chronic constrictive pericarditis may be as follows: The heart is encased in an almost inelastic casing in constrictive pericarditis. In systole and early diastole negative intrapleural pressure (Ppl) may be transmitted to the heart as it is empty. But the heart fills near to its full capacity in early diastole as evidenced by the dip and plateau pattern of ventricular pressure tracing in constrictive pericarditis.
Once filled, it is not possible to distend it further in response to negative intrapleural pressure in inspiration. This can explain the lack of inspiratory decrease in jugular venous pressure in constrictive pericarditis, but not the inspiratory increase. T E Meyer, P Sareli, R H Marcus, W Pocock, M R Berk and M McGregor [2] provided experimental evidence that the inspiratory rise in jugular venous pressure in constrictive pericarditis is in fact due to an “inspiratory hepatojugular reflux phenomenon” as suggested by Hitzig earlier [3]. Meaning that the inspiratory increase in jugular venous pressure in constrictive pericarditis is likely to be the direct consequence of an inspiratory increase in abdominal pressure. This increase is transmitted through an already distended venous system to a heart that is unable to distend further beyond early diastole. Meyers et al had studied abdominal pressures in relation to venous pressures. They noted that the inspiratory rise was not seen when the intra abdominal pressures did not vary much in quiet respiration. But deep inspiration or abdominal corset which increased abdominal pressure caused a parallel inspiratory rise in venous pressure. They also noted rise in right atrial pressure (Pra) with an abdominal corset and a parallel fall in right atrial pressure with fall of abdominal pressure after drainage of tense ascites.
References
- Kussmaul A. Ueber schwielige Mediistino-Pericarditis und den paradoxen puls. Berl Klin Wochenxhr 1873:10:445-449.
- T E Meyer, P Sareli, R H Marcus, W Pocock, M R Berk, M McGregor. Mechanism underlying Kussmaul’s sign in chronic constrictive pericarditis. Am J Cardiol. 1989 Nov 1;64(16):1069-72.
- Hitig WM. On mechanisms of inspiratory filling of the cervical veins and pulsus paradoxus in venous hypertension. J Mount Sinai Harp NY 2942;8.625-644.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal