Cardiology MCQ – Anticoagulation in pregnancy Best maternal outcomes in mechanical prosthetic valves with pregnancy is obtained with: Low molecular weight heparin Heparin Warfarin Dabigatran Click here for
ECG Quiz 60 – Discussion Click here for a larger image In most of the leads, the tracing looks like ventricular fibrillation. QRS complexes are seen very well
Cardiology MCQ – Initial Prosthetic Valve – Answer Initial implantation of a prosthetic valve for treatment of valvular heart disease by Charles Hufnagel in 1952 was into which
Cardiology MCQ – Initial Prosthetic Valve Initial implantation of a prosthetic valve for treatment of valvular heart disease by Charles Hufnagel in 1952 was into which position? Aortic
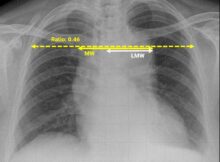
X-ray Quiz 11 – Discussion X-ray chest shows aortic enlargement. Possibilities to be considered are aortic aneurysm, aortic dissection and unfolding of aortic arch in the elderly. In
Risk factors for stent thrombosis Prior stent thrombosis is an important risk factor for future stent thrombosis as well. Diffuse multivessel disease, especially in the presence of diabetes
Echo Quiz – Discussion RA: Right atrium; LA: Left atrium; RV: Right ventricle; LV: Left ventricle; AML: Anterior mitral leaflet; PML: Posterior mitral leaflet This echocardiogram in apical