Rheumatic tricuspid regurgitation
Rheumatic tricuspid regurgitation
Rheumatic tricuspid regurgitation is almost always associated with mitral valve disease. Organic tricuspid regurgitation is often superimposed on hypertensive tricuspid regurgitation which occurs due to pulmonary arterial hypertension secondary to mitral valve disease. Tricuspid leaflets are thickened and deformed by the rheumatic process which leads to incomplete coaptation and tricuspid regurgitation.
Clinically tricuspid regurgitation is manifest as prominent systolic wave in the jugular venous pulse (cv wave) and a pansystolic murmur in the tricuspid area, increasing on inspiration (Carvallo’s sign). Carvallo’s sign may be absent when there is severe heart failure. This is because there is no significant respiratory change when the right heart is already grossly congested. Similar situation occurs when there is associated tricuspid stenosis with high right atrial pressure. Systolic hepatic pulsations are felt in severe tricuspid regurgitation. Associated signs of pulmonary hypertension (palpable and loud pulmonary component of second heart sound or P2) and left parasternal heave due to right ventricular hypertrophy.
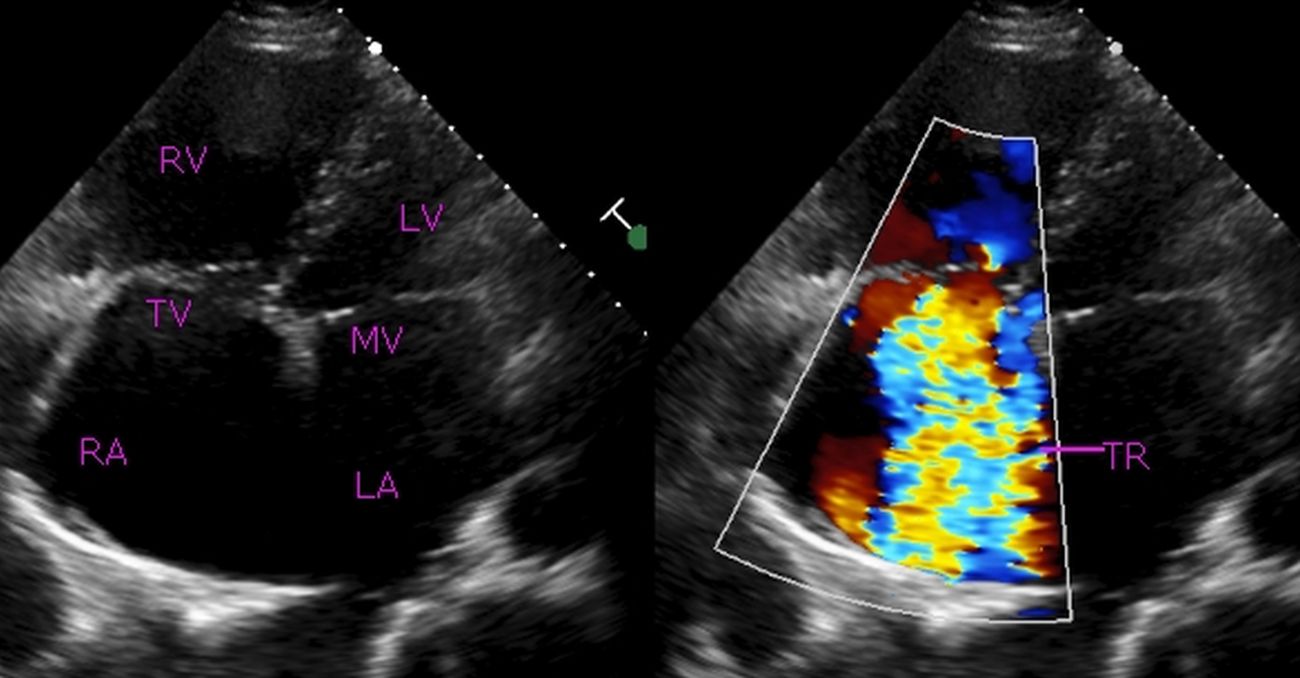
Echocardiogram in severe tricuspid taken in the apical four chamber view: Severe tricuspid regurgitation (TR) is seen as a large mosaic (multi-colored) jet filling more than half of a dilated right atrium (RA). Right ventricle (RV) is also dilated. TV: Tricuspid valve, LV: Left ventricle, MV: Mitral valve, LA: Left atrium.
While hypertensive tricuspid regurgitation may recover once the mitral valve lesion is addressed by valvotomy, repair or valve replacement, organic component of tricuspid regurgitation remains. It may be often difficult to assess how much of the tricuspid regurgitation is organic and how much is likely to reverse after mitral procedure.
Trans catheter repair of tricuspid valve in high surgical risk candidates are being reported. Earlier repair of tricuspid valve was using a Carpentier annuloplasty ring. This used to be done mostly during open heart surgery for repair or replacement of left sided heart valves, usually mitral and seldom as a standalone procedure. Most cases of severe tricuspid regurgitation needing repair are secondary to mitral valve disease and severe pulmonary hypertension and hence this approach was fairly frequent. Tricuspid annuloplasty can also be done without using a ring, known as De Vega procedure.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal