Rotational Atherectomy
Percutaneous transluminal coronary rotational atherectomy
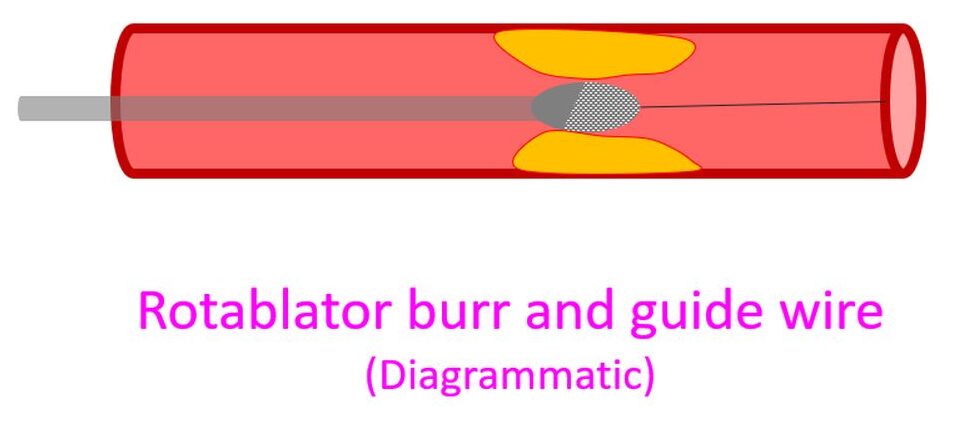
Percutaneous transluminal coronary rotational atherectomy is the technique by which a diamond coated burr rotating at high velocity of 150,000 to 200,000 rpm is used to pulverize the atherosclerotic plaque into tiny particles, usually smaller than the red blood cells. Rotational atherectomy is useful mainly for debulking of calcified lesions which would otherwise not yield even to high pressure balloon inflations. The basic equipment used is called the rotablator console.
Stent dilatation and good apposition to vessel wall are not feasible in heavily calcified lesions. Such poorly apposed stents tend to develop stent thrombosis, may cause stent fracture or restenosis. Even high pressure non compliant balloon inflations may be unable to crack calcified lesions to adequately prepare a heavily calcified vessel for optimal stent delivery [1].
Rotablation removes the calcification and modifies the calcified atherosclerotic plaque vessel wall compliance. Lumen gain with rotational atherectomy is much more compared to simple balloon angioplasty. Rotablator is the most commonly used atherectomy device. It removes calcified plaques using microscopic diamond chips embedded on a rapidly rotating olive shaped burr [1].
The disposables used for each case are the advancer, rota burr and the rota guide wire. Rotation of the burr needs high pressure compressed air or nitrogen. The console has a tachometer which displays the rotational speed. Turbine pressure gauge displays the pressure delivered to the advancer. The floppy guide wire used for rotablator has a length of 325 mm with a 22 mm soft spring tip. The extra support guidewire has a 28 mm soft spring tip.
Reference
- Pedro J Valdes, Shivaraj Nagalli, Miguel A Diaz. Rotational Atherectomy. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal