ST elevation during treadmill test
ST elevation during treadmill test
Usual ischemic response on a treadmill ECG is ST segment depression. But sometimes ST segment elevation may also be noted. ST segment depression seen during treadmill test (TMT) does not have localizing value regarding the territory of ischemia. But ST elevation is thought to have localizing value. ST segment elevation occurring in leads with Q waves was initially thought not to represent ischemia and rather a manifestation of a dyskinetic segment. But now ST segment elevation in leads with Q waves is thought to be a sign of viability in the infarct territory. In this series, there is ST segment elevation in the inferior leads with Q waves as well as ST depression in I and aVL, persisting well into recovery. In some cases during treadmill test, ST segment depression does not appear during exercise, but only in recovery. In still others, ST segment depression is mild and horizontal during the exercise, but worsens in recovery, often becoming down sloping. All these changes are quite significant and are considered indications for coronary angiography.
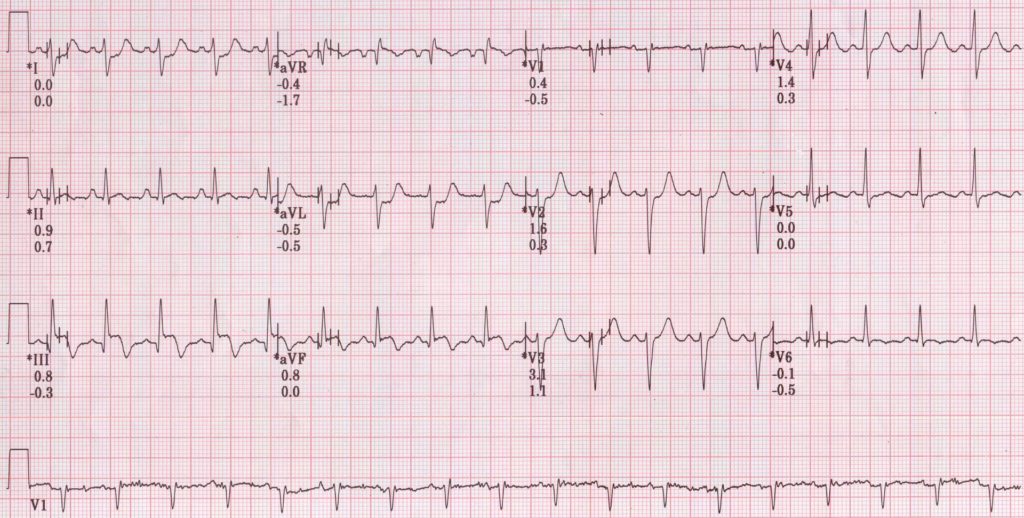
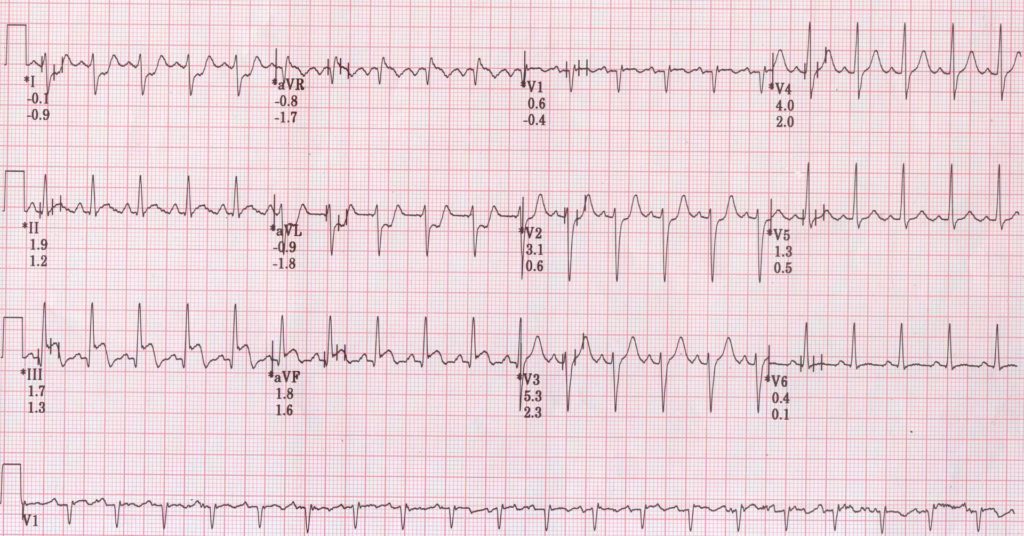
TMT stage 2 showing ST elevation in inferior leads and ST depression in lead I and aVL
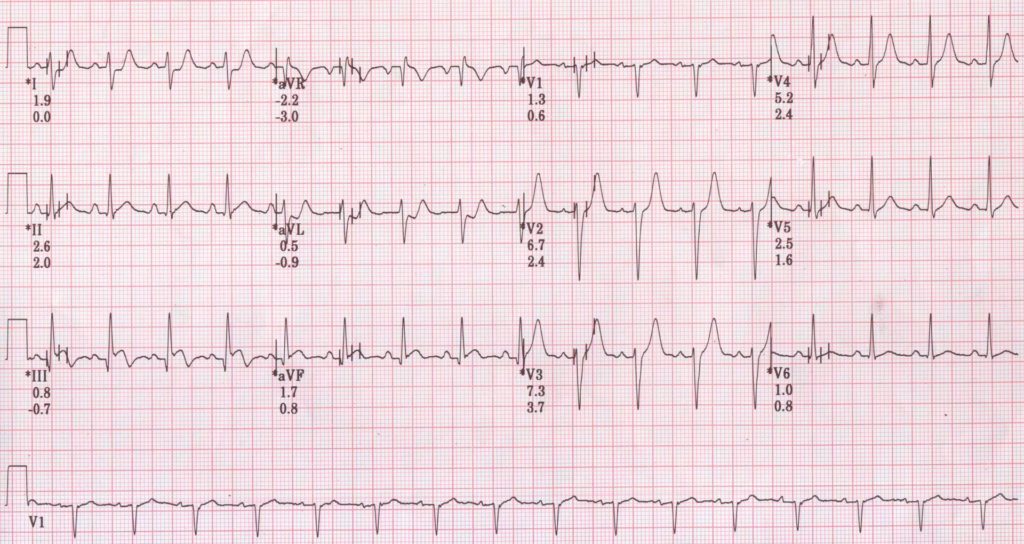
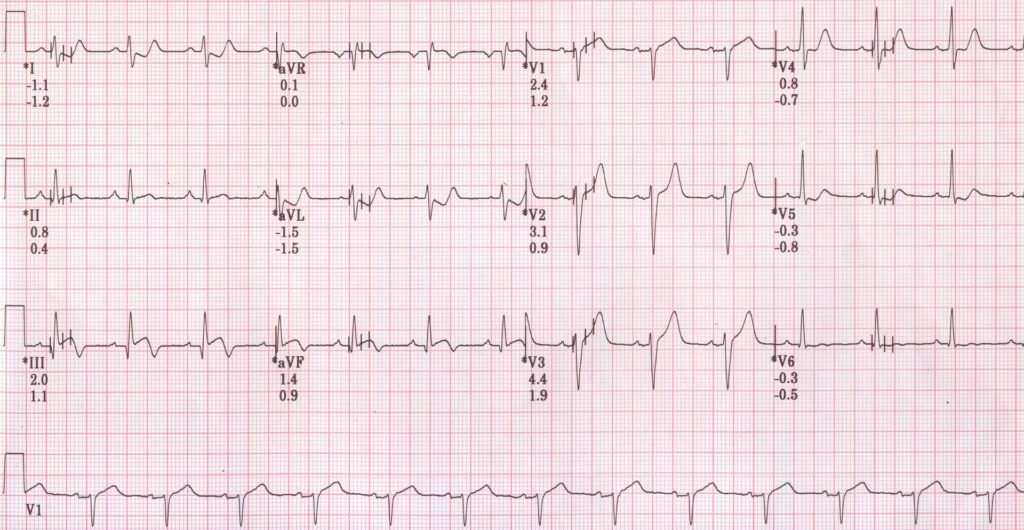
TMT recovery at 2 minutes showing ST elevation in inferior leads and mild ST depression in lead I and aVL.
Miyakoda H et al studied the causes of ST segment elevation during exercise test [1]. 15 of their patients had previous anterior wall infarction, but coronary angiogram showed less than 75% narrowing (Group I). 36 of their patients had effort angina and 90% or more narrowing of left anterior descending coronary artery (LAD) and no previous myocardial infarction (Group II). All the group I patients had exercise induced ST elevation, but no Thallium 201 (201Tl) redistribution. In group II, only those with 99% narrowing of LAD and poor collaterals, showed exercise induced ST segment elevation. None of those with total occlusion or 99% narrowing with good collaterals or those with 90% narrowing showed exercise induced ST elevation. Those with exercise induced ST elevation showed lower 201Tl uptake during exercise and washout in the territory of the diseased vessel than in those without exercise induced ST elevation. They concluded that exercise induced ST elevation can occur due to wall motion abnormalities in the absence of myocardial ischemia. In those with effort angina, exercise induced ST elevation indicated severe coronary obstruction with poor collaterals and severe myocardial ischemia.
Precordial ST elevation with exercise has been reported in severe pulmonary hypertension without coronary artery disease [2]. Authors proposed right ventricular dilatation as the possible cause of ST segment elevation.
ST segment elevation during recovery phase of treadmill test with hypotension and normal coronaries on emergency angiogram has also been documented [3]. The authors presumed that coronary spasm would have been the reason in that case.
In another case report, isolated ST segment elevation in aVR with exercise at high workload (10.21 Mets) was shown to be due to ostioproximal LAD occlusion [4]. The patient had good collaterals from right coronary artery, explaining the good effort tolerance.
References
- Miyakoda H, Kato M, Noguchi N, Omodani H, Osaki S, Matsumoto T, Kinugawa T, Hoshio A, Kotake H, Mashiba H. Exercise-induced ST-segment elevation–role of left ventricular wall motion abnormalities and coronary artery narrowing. Jpn Circ J. 1995 Nov;59(11):725-35.
- Nguyen TH, Clavijo LC, Naqvi TZ. Acute ST segment elevation during exercise stress echocardiography due to severe pulmonary hypertension. Cardiovasc Ultrasound. 2011 Jun 6;9:18.
- Aghamohammadzadeh R, El-Omar SM, Rowlands D, El-Omar M. ST elevation in recovery post exercise with normal coronary arteries. BMJ Case Rep. 2019 Jul 8;12(7):e229766.
- Hirapur I, Mantgol RV, Agrawal N. Isolated ST elevation in lead aVR during TMT at high workload as a marker of ostioproximal LAD occlusion. BMJ Case Rep. 2014 Mar 18;2014:bcr2013203171.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal