Polymorphic VPC and NSVT on Holter
Polymorphic VPC and NSVT on Holter
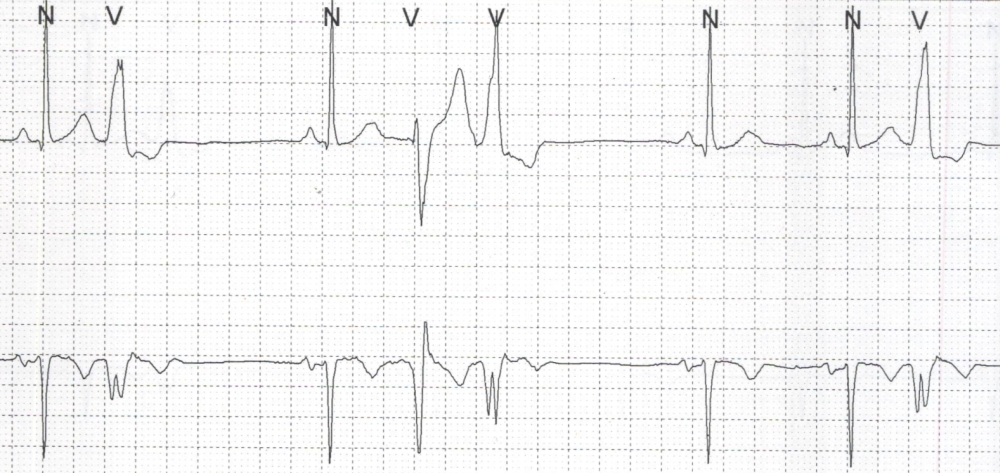
First complex is a sinus beat with narrow QRS and a preceding P wave with a normal PR interval. The second beat is premature complex with wide QRS and no preceding P wave. It is a ventricular premature complex (VPC). In the upper panel, the ST segment of the VPC is depressed and T wave inverted. The VPC is followed by a pause (compensatory pause). The third beat is again a sinus beat, while fourth and fifth beats are wide QRS complexes without preceding P waves. But the QRS deflection is negative for one and positive for the other. This should suggest that they are possibly originating from two different foci. The first VPC of the couplet is about 200 milliseconds after the T wave of the preceding beat while the second VPC is just beyond the end of the preceding T wave. The second VPC is followed by a pause and two consecutive sinus beats. The last beat is again VPC. Three VPCs have similar morphology (monomorphic) while one VPC has a different morphology. Polymorphic VPCs and short coupled VPCs are thought to be fore runners of more complex arrhythmias.
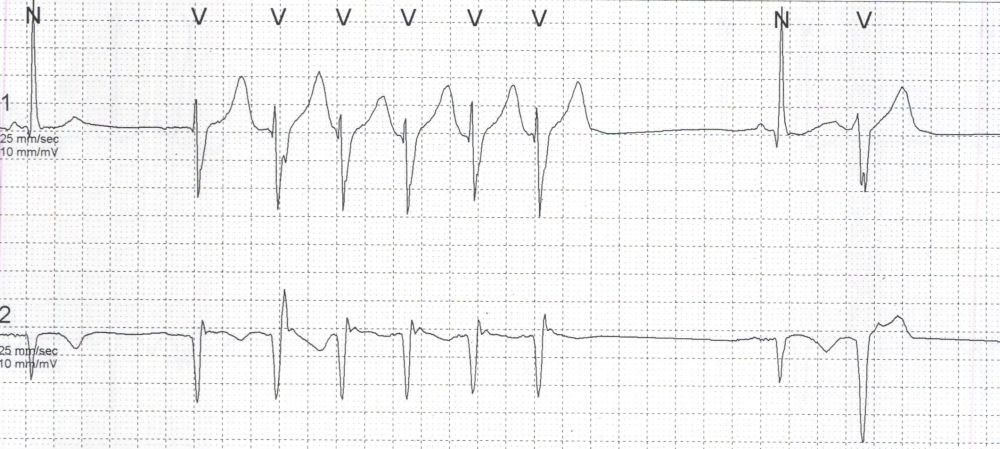
The first beat in this sequence is a narrow QRS complex with a preceding P wave and a normal PR interval, suggesting sinus beat. After a pause, there is run of wide QRS complexes, which can be called a non sustained ventricular tachycardia (NSVT). The beats are not preceded by definite P waves. But there is some difference in the shapes of T waves. The interval between the first and second beats of the tachycardia run is more that of the subsequent intervals. The tachycardia run is followed by a pause before the next sinus beat appears. The last beat is an early VPC. It interesting to note that the tachycardia does not start with an early VPC. The clinical setting was in a person with old inferior wall myocardial infarction with a chronic total occlusion of the right coronary artery. The arrhythmia could be arising from the left ventricular scar. The ventricular tachycardia from this region usually has a morphology similar to posterior fascicular ventricular tachycardia (Belhassen’s VT) with right bundle branch morphology in V1 with left axis deviation. Differentiation of this type of scar VT from posterior fascicular VT is important because the former is more difficult to ablate while the ablation can be considered as the treatment of choice for the latter. In this case, though the tachycardia appears to be monomorphic, the VPCs are polymorphic, which may suggest more than once foci.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal