TR Jet on CW Doppler
TR Jet on CW Doppler
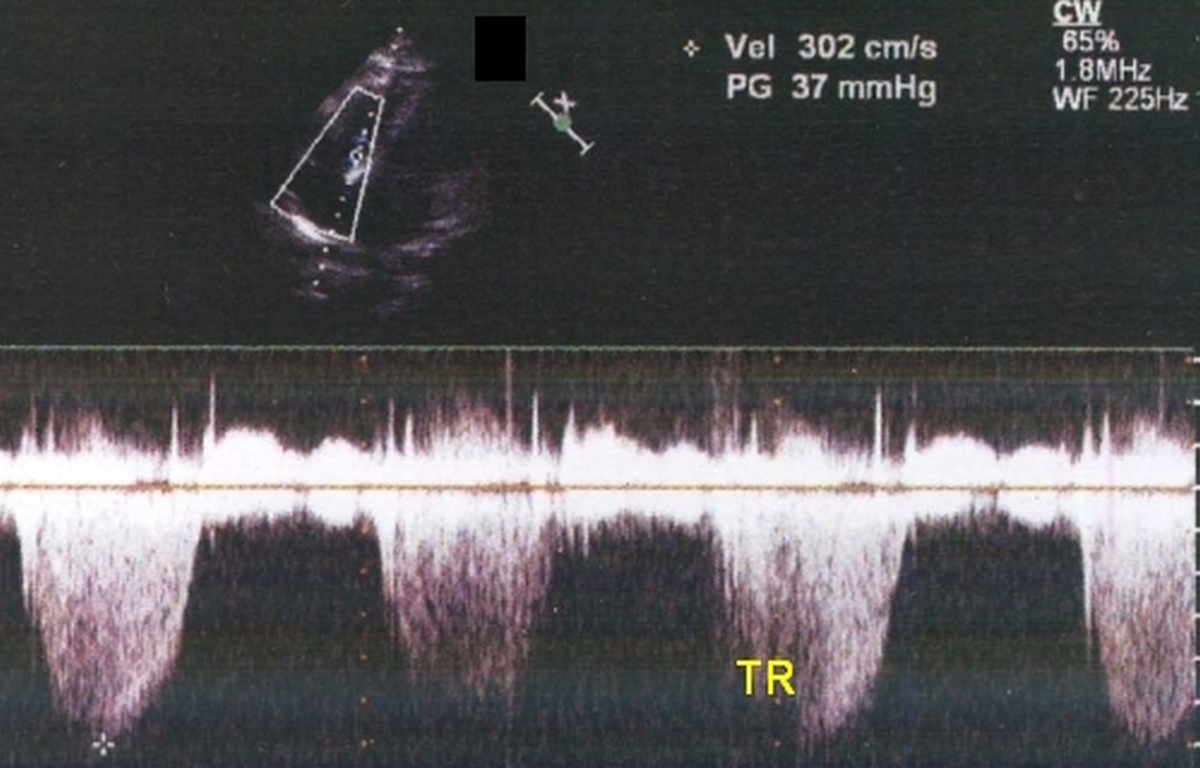
Tricuspid regurgitation jet on continuous wave Doppler: Continuous wave (CW) Doppler interrogation from the apical four chamber view for echocardiography across the tricuspid valve picked up this jet with a velocity of 302 cm/s and a peak gradient (PG) of 37 mm Hg. Gradient is calculated from the velocity using modified Bernoulli’s equation:
Pressure gradient = 4 V2, where is V is the velocity of the jet.
If the right atrial pressure is taken as 10 mm Hg (as it is conventionally done), the estimated right ventricular systolic pressure (RVSP) would be 47 mm Hg. If the right atrial pressure is elevated as evidenced by a raised jugular venous pressure (JVP), appropriate corrections may be made for the measured JVP. If the inferior vena cava is plethoric, right atrial pressure will be high and we may add 20 mm Hg instead of 10 mm Hg to get the RVSP. The incomplete envelope in certain cycles is because the heart moves with respect to the Doppler cursor. Changes could also be due to changes in the volume of regurgitation in different phases of respiration. Tricuspid regurgitation increases as the systemic venous return increases in inspiration. Tricuspid regurgitation (TR) is often secondary to right ventricular / pulmonary hypertension as in this case. Sometimes a low pressure TR can occur due to the inherent disease of the tricuspid valve as in carcinoid syndrome or Ebstein’s anomaly. In rheumatic heart disease the mechanism can be a combination of valvular abnormality as well as elevated right ventricular pressures due to pulmonary hypertension secondary to left sided valvular lesions. Severe organic tricuspid regurgitation may require tricuspid annuloplasty.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal