Treatment of acute limb ischemia
Treatment of acute limb ischemia
Acute limb ischemia is a rapid decrease in the blood flow to the limb either due to occlusion of a peripheral artery or a bypass graft. Prompt treatment is required to save the limb as well as life. Important reasons for acute limb ischemia are embolic occlusions and thrombosis of the blood vessel. Major symptoms of acute limb ischemia have been called as the 5 Ps and 6 Ps of critical limb ischemia.
Treatment options for acute limb ischemia vary from open surgical vascular revascularization, endovascular recanalization or a hybrid approach along with administration of heparin. Heparinization is to prevent the proximal and distal progression of secondary thrombosis from the site of occlusion. Very rarely amputation may be needed if there is irreversible ischemia. There is a potential risk of severe ischemia-reperfusion injury if a long time has passed after the occlusion before reperfusion [1].
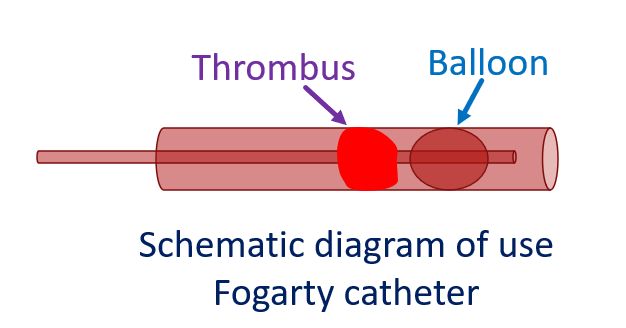
Age old surgical treatment is thromboembolectomy using a Fogarty catheter [2]. Usual protocol is surgical dissection and exposure of the common femoral artery, superficial femoral artery or brachial arteries depending on the case. Supplementary distal access may be used when needed [3]. Bypass surgery is the next option when thromboembolectomy is not feasible or successful.
Endovascular treatment options are catheter directed thrombolysis, percutaneous thrombus aspiration and stent placement. Hybrid treatment combines both treatments. A Cochrane review comparing surgery and thrombolysis, published in 2013 concluded that there is no overall difference in limb salvage or death at one year between initial surgery and initial thrombolysis. But thrombolysis may be associated with a higher risk of ongoing limb ischemia and hemorrhagic complications including stroke [4].
With the availability of hybrid operating rooms, hybrid treatment with endovascular surgery and simultaneous intraoperative angiography for residual lesions after surgical thromboembolectomy is feasible. In the hybrid suite, diagnosis by angiography with initial and additional treatment if needed gives good revascularization. Additional treatment possible are balloon dilatation after thromboembolectomy and stent placement. This is facilitated by over-the-wire type Fogarty catheter and hybrid suites in which even thromboembolectomy is fluoroscopically assisted [1].
References
- Obara H, Matsubara K, Kitagawa Y. Acute Limb Ischemia. Ann Vasc Dis. 2018 Dec 25;11(4):443-448. doi: 10.3400/avd.ra.18-00074. PMID: 30636997; PMCID: PMC6326052.
- Fogarty TJ, Cranley JJ. Catheter technic for arterial embolectomy. Ann Surg 1965; 161: 325-30.
- Teodoro C, Bertanha M, Girard FPCM, Sobreira ML, Yoshida RA, Moura R, Jaldin RG, Yoshida WB. Results of treatment of acute occlusions of limb arteries at a university hospital – retrospective study. J Vasc Bras. 2020 Nov 16;19:e20200031.
- Berridge DC, Kessel DO, Robertson I. Surgery versus thrombolysis for initial management of acute limb ischaemia. Cochrane Database Syst Rev. 2013 Jun 6;(6):CD002784. doi: 10.1002/14651858.CD002784.pub2. Update in: Cochrane Database Syst Rev. 2018 Aug 10;8:CD002784. PMID: 23744596.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal