Ventricular ectopic bigeminy
Ventricular ectopic bigeminy
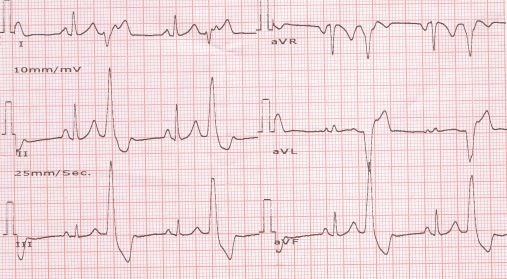
Clinical findings will be pulsus bigeminus and intermittent cannon waves as alternate P waves are falling on the T waves. When P waves fall on the latter part of QRS, ST segment or T waves, cannon waves can be expected as QT interval roughly represents the electrical systole of the ventricle. (Diastole ends and systole starts at the peak of R wave). In the tracing, P waves are seen as distortions in the contour of the T wave of the ectopic beat. The distortion is exactly midway between the preceding and succeeding P waves of the sinus beats (narrow QRS). Ventricular ectopics are characterised by wide bizarre complexes which are premature and not preceded by P wave. The ventricular ectopic beats are followed by a full compensatory pause meaning that the sum of the coupling interval (interval from the onset of the previous QRS to the onset of the ectopic QRS) and the compensatory pause (the next RR interval) will be exactly twice that of the RR interval of sinus beats. The exact compensatory pause is because the sinus cycle is not reset by the ventricular beat as it finds the retrograde path to the sinus node refractory.
Sometimes the retrograde conduction to the AV node produces a prolongation of conduction of the next sinus beat manifesting as a prolongation of the next PR interval (not present in this ECG). This is a manifestation of concealed retrograde conduction.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal