VVI pacing with very wide QRS
VVI pacing with very wide QRS
Interesting ECG
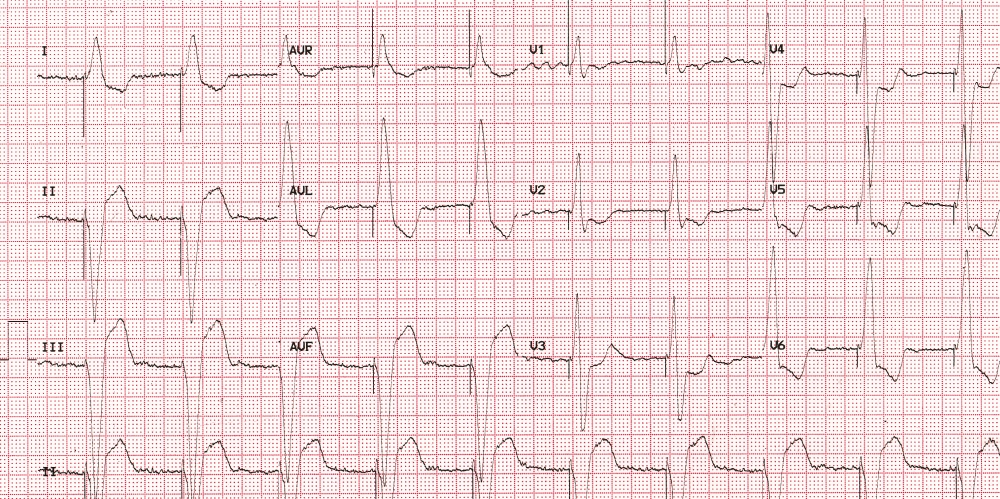
12 lead ECG showing paced rhythm with a very wide QRS
ECG shows a paced rhythm with a wide QRS of 200 milliseconds. A prominent pacing spike is seen before each QRS complex, indicating a ventricular paced rhythm with complete capture. Fibrillary waves are seen in leads V1 and V2. Hence the underlying rhythm at present is atrial fibrillation. The fact that the pacemaker has been implanted would suggest that there was an indication for pacing earlier.
In this case the patient had complete heart block earlier and permanent pacemaker was implanted. Later the person developed atrial fibrillation and the regular P waves usually seen with complete heart block were replaced by fibrillary waves. Left ventricular dysfunction and consequent atrial dilatation, could account for the relatively coarse fibrillary waves.
The enhanced width of the QRS indicates higher amount of myocardial damage which has led to the ventricular dysfunction and a more disorganised intraventricular conduction. The wide QRS with left bundle branch block pattern in right ventricular pacing could worsen the left ventricular function by intraventricular dyssynchrony between the contractions of the interventricular septum and left ventricular lateral wall.
This is one of the downsides of right ventricular apical pacing. The apical location of the pacing site is evident from the negative QRS complexes in the inferior leads. This disadvantage of right ventricular apical pacing in terms of dyssynchrony and progressive worsening of left ventricular function have prompted investigators to look at options like right ventricular outflow septal pacing, direct His bundle pacing, left bundle branch pacing and even biventricular pacing in order to prevent this vicious cycle. Various pacing algorithms to minimize ventricular pacing in cases of sick sinus syndrome are also in use while pacing from the right ventricular apex in those who are not pacemaker dependant.
Another possibility to be considered when atrial fibrillation is seen in a paced ECG is the implantation of a pacemaker after ablation of the AV node in refractory atrial fibrillation in which rate control with drugs have either failed or has produced intolerable side effects.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal