Left ventricular aneurysm and pulmonary hypertension
Left ventricular aneurysm and pulmonary hypertension
Left ventricular aneurysm and pulmonary hypertension noted on X-ray chest PA view. This is the non-annotated image. Annotated image follows.
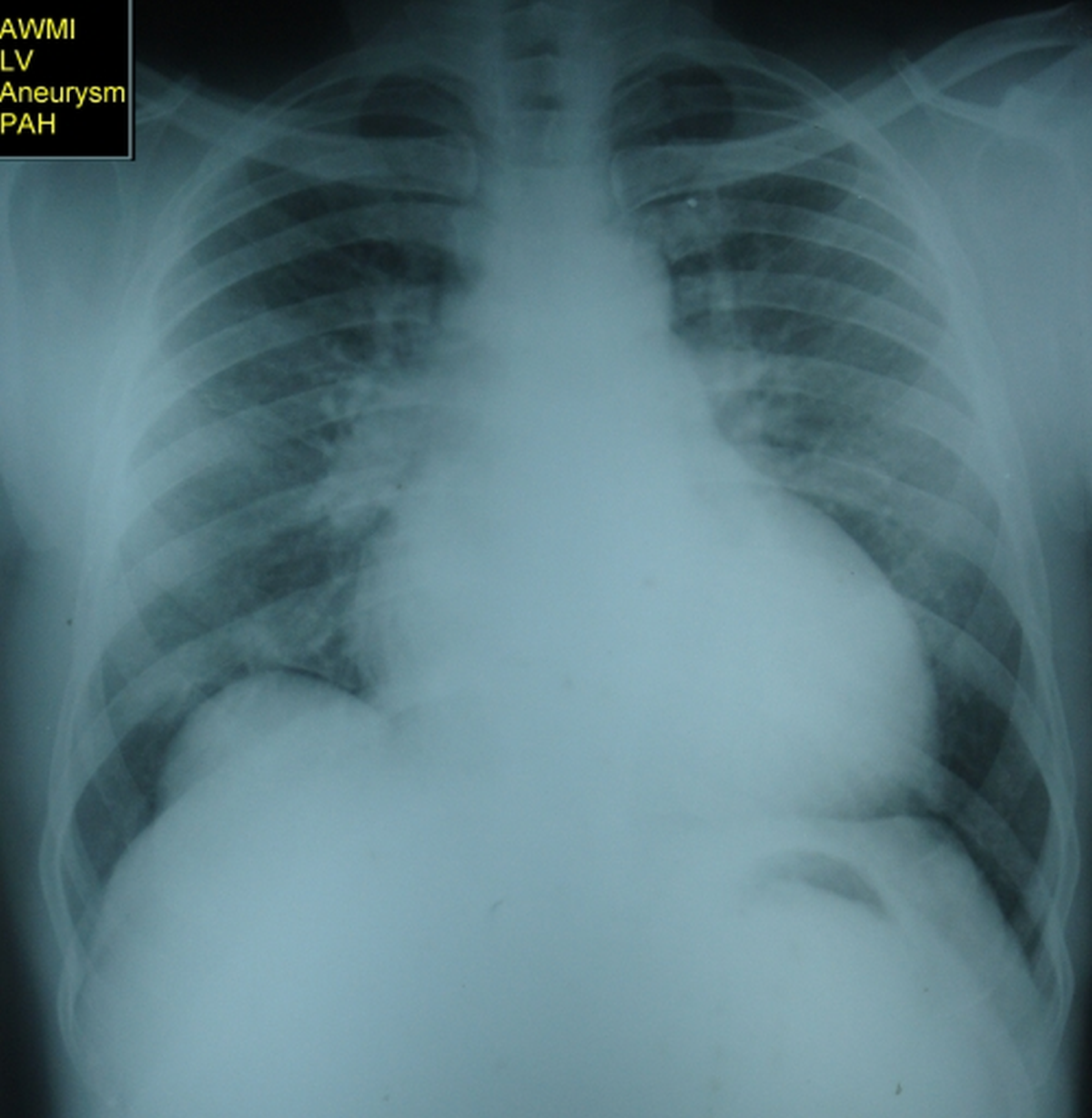
(See annotated image below)
Anterior wall myocardial infarction, LV aneurysm and pulmonary hypertension, both venous and arterial were present. There is cardiomegaly with a bulge along the left cardiac border above the apex, indicating a left ventricular aneurysm. Clinically there was a dyskinetic pulsation in this region over the chest. Main pulmonary artery is prominent and right pulmonary artery is large due to pulmonary hypertension. Prominent upper lobe vessels are seen, especially on the left side, suggesting pulmonary venous hypertension secondary to left ventricular failure and elevated left ventricular end diastolic pressure which is common with LV aneurysm.
Prominent upper lobe vessels due to pulmonary venous hypertension have multiple names like antler sign, inverted mustache sign, cephalization and redistribution. Normally lower lobe vessels are more prominent due to the effect of gravity.
Right border of the heart is shifted to the right indicating right atrial enlargement. Close scrutiny shows a shadow within shadow or double atrial shadow, suggesting associated left atrial enlargement.
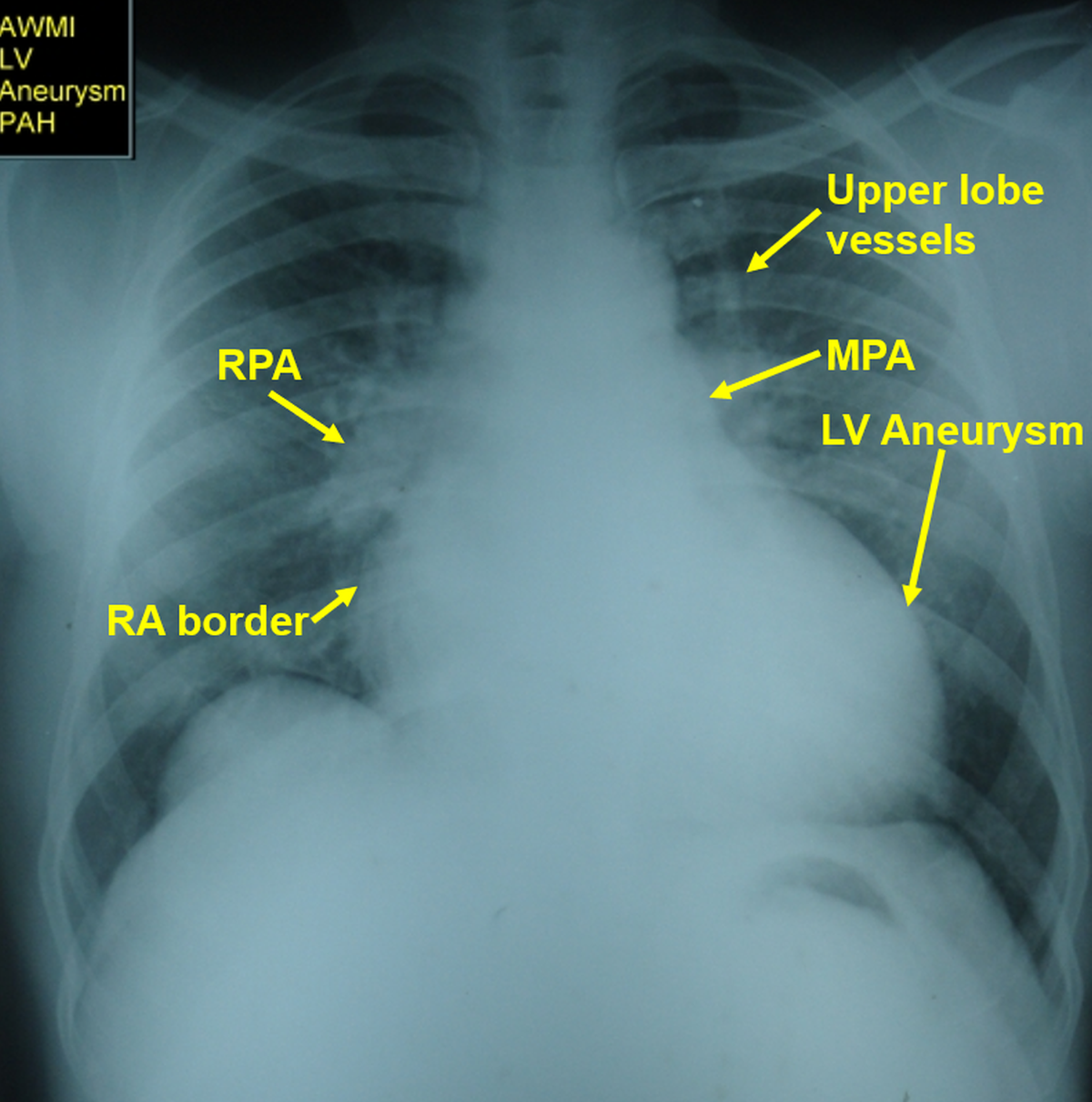
RA: Right atrium; RPA: Right pulmonary artery; MPA: Main pulmonary artery; LV Aneurysm: Left ventricular aneurysm
Two important complications of left ventricular aneurysm other than heart failure are the formation of mural thrombus and recurrent ventricular tachycardia. Though the mural thrombus is less likely to embolize being in a dyskinetic region, it is conventional to give anticoagulation if there is a mural thrombus, with all precautions. Recurrent ventricular tachycardia is due to reentrant circuits in the border zone between the aneurysm and adjacent tissue where there is viable myocardium producing conduction channels. Catheter ablation is an option in drug refractory cases [1].
Reference
- Jin-Rui Guo, Li-Hui Zheng, Ling-Min Wu, Li-Gang Ding, Yan Yao. Aneurysm-related ischemic ventricular tachycardia: safety and efficacy of catheter ablation. Medicine (Baltimore). 2017 Mar;96(13):e6442.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal