Hypertrophic cardiomyopathy (HCM) with mild AR – echocardiogram
Hypertrophic cardiomyopathy (HCM) with mild AR – echocardiogram
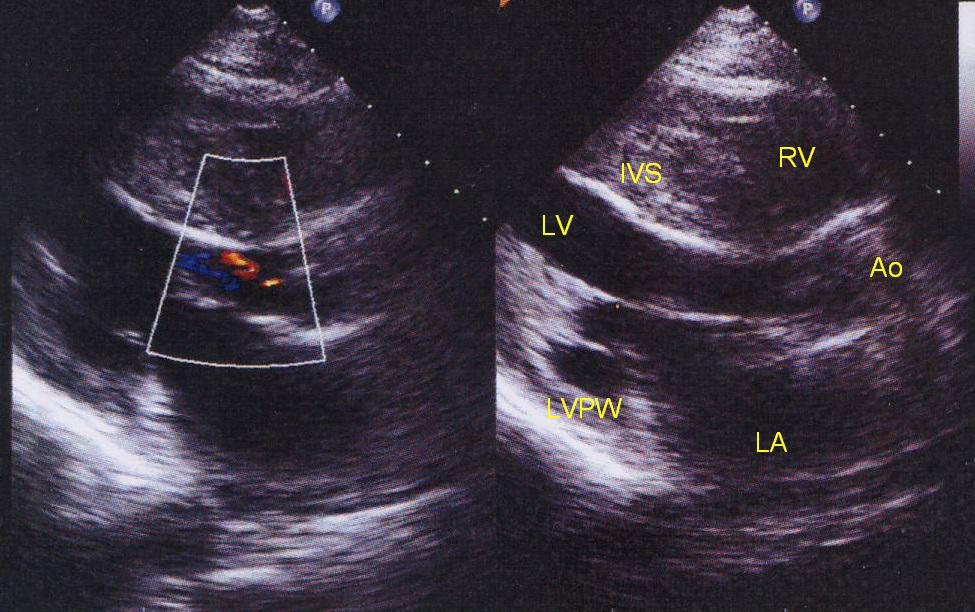
Echocardiogram in parasternal long axis view showing the asymmetric septal hypertrophy. The interventricular septum (IVS) is much thicker than the left ventricular posterior wall (LVPW). Septal to posterior wall ratio of more than 1.5 is highly suggestive of hypertrophic cardiomyopathy (HCM). Here the septum is more than twice as thick as the posterior wall. In addition to asymmetric hypertrophy, septal systolic thickening will be reduced. LV: left ventricle; LA: left atrium; RV: right ventricle; Ao: aorta.
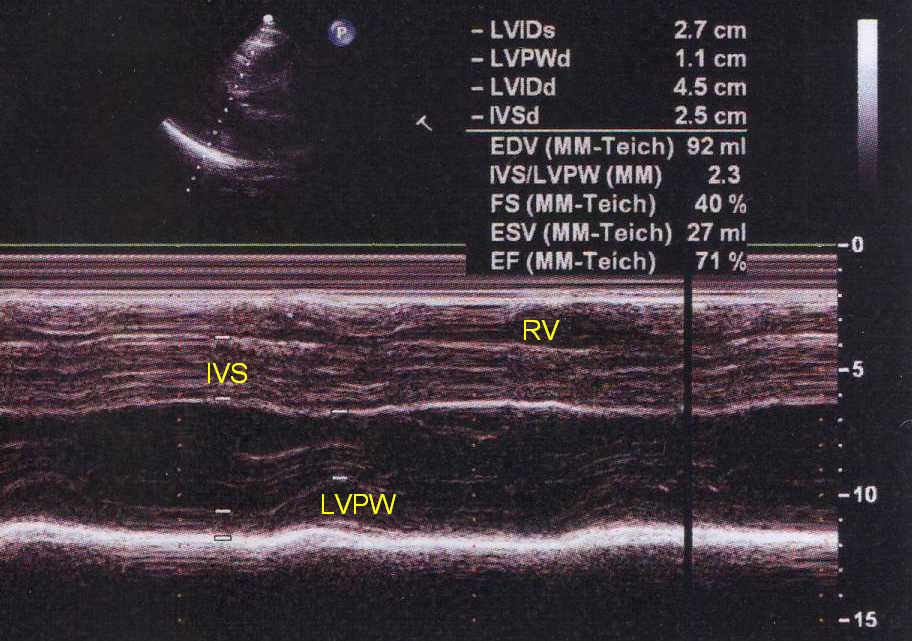
M-Mode tracing from the parasternal view showing a thickened interventricular septum (IVS) with poor systolic thickening. Note that change in thickness of the IVS in systole is less than that of the left ventricular posterior wall (LVPW). Left ventricular cavity is typically small in HCM. LVIDs: left ventricular internal diameter in systole; LVPWd: left ventricular posterior wall in diastole; LVIDd: left ventricular internal diameter in diastole; IVSd: interventricular septum in diastole; EDV: end diastolic volume; IVS/LVPW: interventricular septum to left ventricular posterior wall ratio (diastolic); FS: fractional shortening (of left ventricle); ESV: end systolic volume (left ventricle); EF: ejection fraction (left ventricle). The septal to posterior wall ratio in this case is 2.3. The ejection fraction here is 71% (normal) as there is no systolic dysfunction in HCM, except in the very late dilated phase.
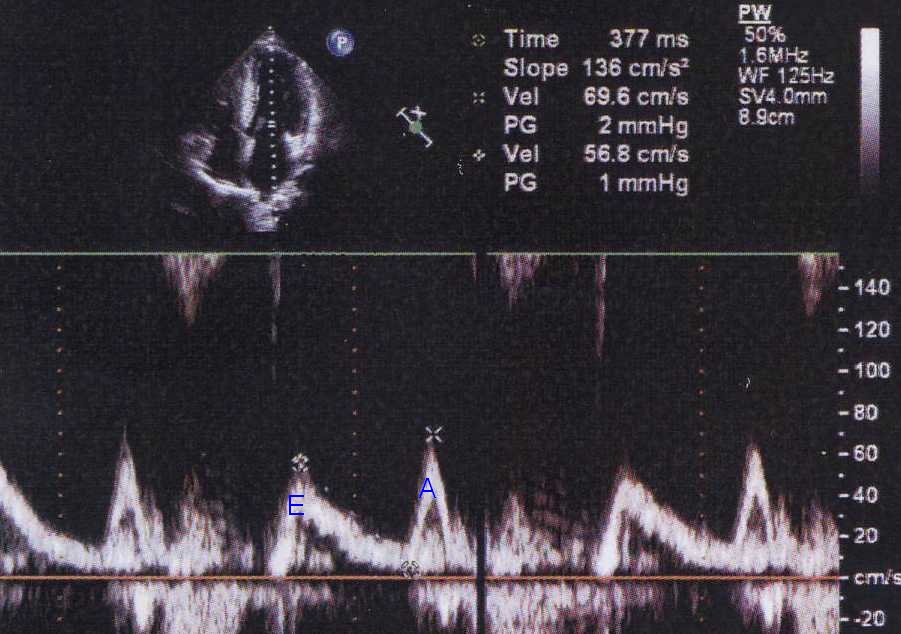
The E wave represents early diastolic filling of the left ventricle and the A wave the atrial systolic filling. Normally most the E wave is taller than the A wave. In HCM and other conditions with a stiff left ventricle, the atrial contribution to ventricular filling is increased. Hence the A wave becomes taller than E wave (E/A reversal), one of the simple Doppler echocardiographic findings of left ventricular diastolic dysfunction. This finding is quite common in older individuals with lusitropic abnormality (impaired relaxation) of the left ventricle. In this case the A wave peak velocity is 69.6 cm/sec corresponding to a calculated peak gradient (PG) of 2 mm Hg and the E wave peak velocity is 56.8 cm/s.
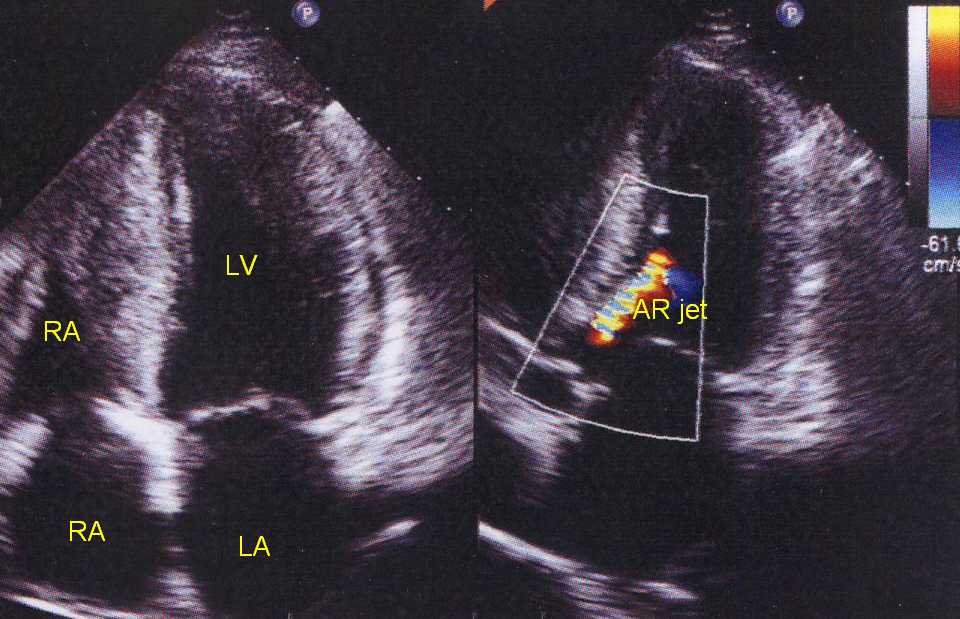
Apical four chamber view (left) and apical five chamber view (right) showing mild aortic regurgitation by colour flow mapping (CFM). AR jet is a mosaic (multi-coloured) jet due to aliasing as seen in all high velocity jets. The gross hypertrophy of the interventricular septum is also seen in the left panel.
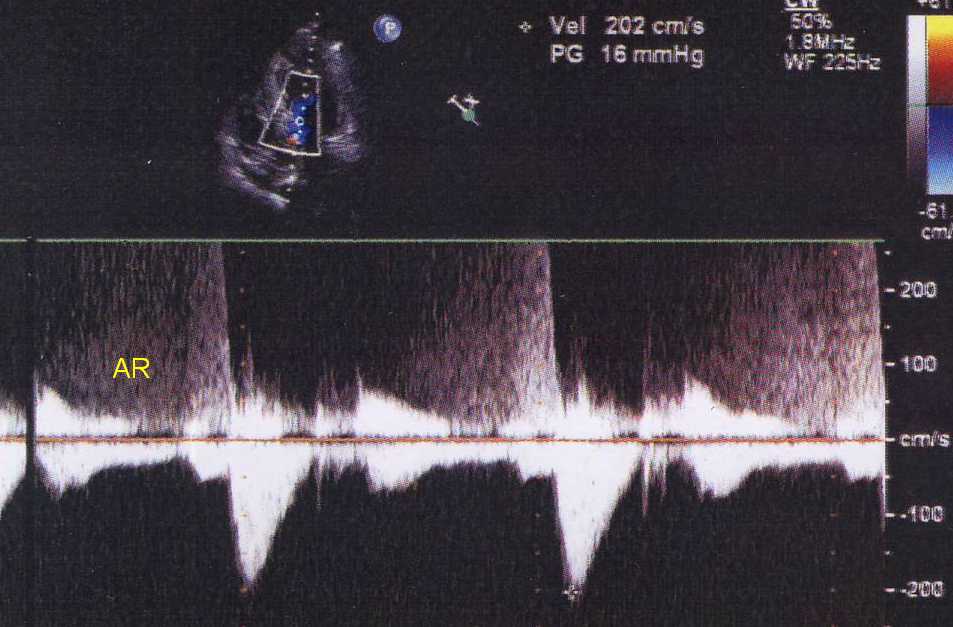
Continuous wave Doppler interrogation of aortic flow from apical five chamber view showing aortic forward flow (dense downward signal) and regurgitant flow (AR) towards the transducer. The regurgitant signal is faint as the regurgitation is not severe. Upper portion of the signal is clipped as the velocity is more that for the imaging system. In mild regurgitation the envelope of the regurgitant signal is incomplete as in this case. The gradient (PG) shown is for the forward signal and is 16 mm Hg, with a velocity (Vel) of 202 cm/s indicating that there is no significant aortic stenosis.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal