Paradoxical splitting of second heart sound
Paradoxical splitting of second heart sound
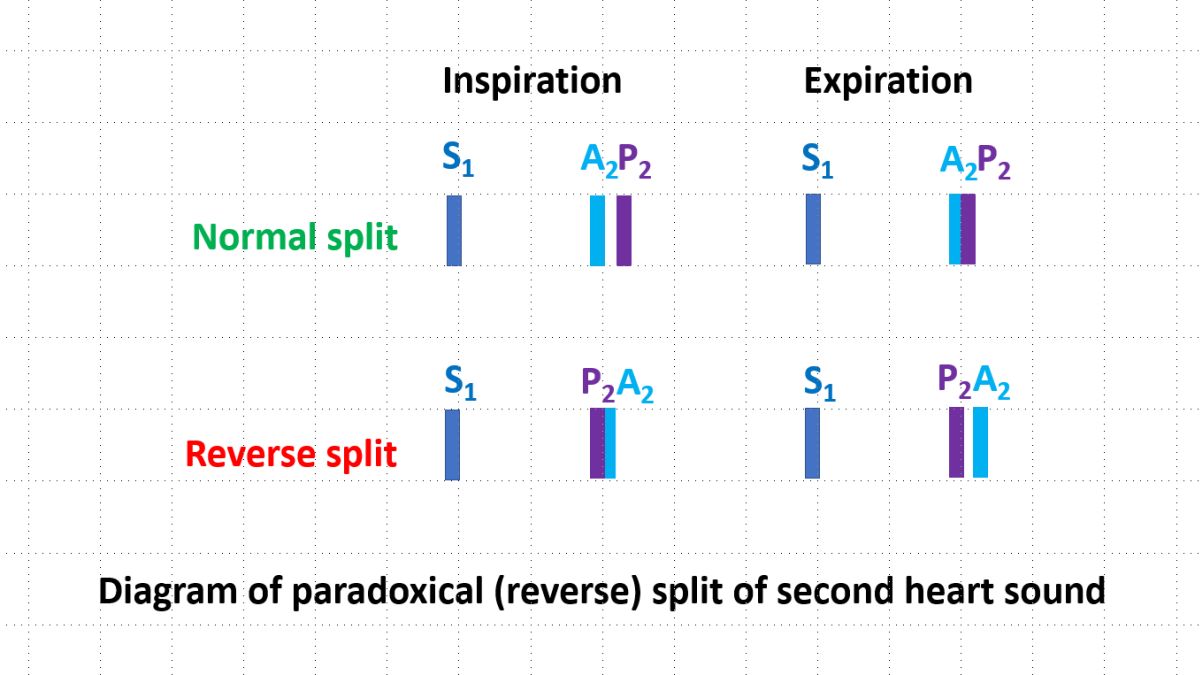
Normal split of second heart sound is due to the delay in pulmonary valve closure compared to aortic valve. This is mostly contributed to by the pulmonary hang out interval. Hang out interval is the time taken for the actual valve closure after the pulmonary artery and right ventricular pressure tracings crossover. Normal split of second heart sound closes in expiration as the reduced venous return shortens right ventricular ejection. When the split closes in inspiration and becomes audible in expiration, it is called paradoxical splitting of second heart sound. Please note that a wide split of second heart sound as in right bundle branch block or atrial septal defect will be audible in expiration. But it is also heard in inspiration, unlike a paradoxical split which closes in inspiration. An audible expiratory split may also be heard in young individuals in supine position. This physiological expiratory split closes in sitting and standing positions [1].
Paradoxical splitting of second heard sound can also be called reversed splitting. It is due to the delay in the aortic valve closure sound. In normal split of second heart sound, aortic component (A2) occurs first and is followed by pulmonary component (P2). The sequence of A2-P2 is reversed to P2-A2 in reverse splitting or paradoxical splitting.
Paradoxical splitting is seen only in pathological conditions. Most common cause of paradoxical splitting of second heart sound is left bundle branch block, in which aortic closure is delayed due to the delay in left ventricular activation. Paradoxical splitting in aortic stenosis indicates severe aortic stenosis causing delay in A2. Other important cause of left ventricular outflow obstruction, hypertrophic obstructive cardiomyopathy also causes paradoxical split of S2. Severe left ventricular dysfunction with delayed emptying of left ventricle is another cause of reverse split of second heart sound. Right ventricular ectopic beat, right ventricular paced beat [2] and right ventricular pre-excitation [3] can also theoretically cause a paradoxical splitting of second heart sound due to earlier activation of right ventricle and delayed activation of left ventricle. All these conditions resemble left bundle branch block on the ECG. Paradoxical splitting of second heart sound has been reported in 10 out of 29 cases of patent ductus arteriosus in a study [4]. Authors mentioned that it was due to difference between right and left ventricular systolic times as in aortic stenosis.
In an interesting case report, late systolic click from isolated tricuspid valve simulated paradoxical splitting of second heart sound [5]. Echocardiography with simultaneous phonocardiography was used to demonstrate this phenomenon. Respiratory variation of the tricuspid valve click in relation to the second heart sound resulted in this auscultatory phenomenon which resembled reverse splitting of second heart sound.
References
- Felner JM. Chapter 23. The Second Heart Sound. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Walker HK, Hall WD, Hurst JW, editors. Boston: Butterworths; 1990.
- Towne WD, Rahimtoola SH, Sinno MZ, Loeb HS, Rosen KM, Gunnar RM. The effects of right atrial and ventricular pacing on the auscultatory findings in patients with mitral valve prolapse. Circulation. 1975 Jun;51(6):988-96.
- Ito M, Fujino T, Kanaya S, Imanishi S, Mashiba H. Phono-, echo-, and electro-cardiographic correlation in the Wolff-Parkinson-White syndrome, with special reference to the split pattern of second heart sound. Jpn Heart J. 1977 May;18(3):329-39.
- GRAY IR. Paradoxical splitting of the second heart sound. Br Heart J. 1956 Jan;18(1):21-8.
- Farrar MW, Engel PJ, Eppert D, Plummer S. Late systolic click from isolated tricuspid valve prolapse simulating paradoxical splitting of the second heart sound. J Am Coll Cardiol. 1985 Mar;5(3):793-6.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal