Segmental approach to congenital heart disease
Segmental approach to congenital heart disease
Segmental approach is used routinely in the echocardiographic evaluation of congenital heart disease. It is also useful in other cardiac imaging modalities used for evaluation of congenital heart disease like computed tomography and magnetic resonance imaging. Chest X-ray is useful in evaluating the cardiac position and visceral situs as it gives an overview of cardiac position in the thorax, position of left and right bronchi, aortic arch, liver and stomach air bubble [1].
Here is a chest X-ray in mesocardia with levo transposition of great arteries:

Here is another chest X-ray showing right aortic arch in tetralogy of Fallot:
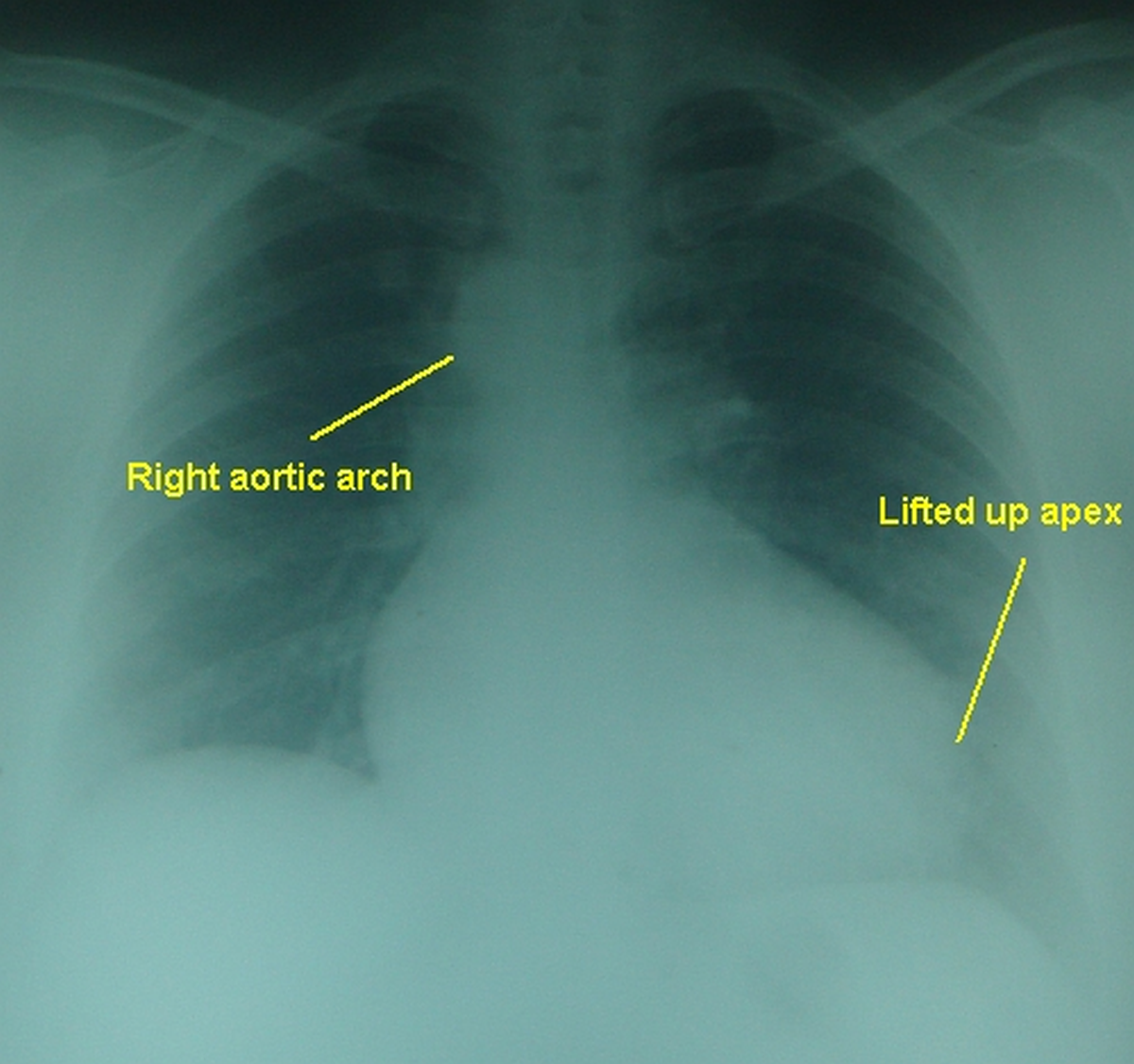
In both these cases, the visceral situs is solitus, as the stomach air bubble is on the left side and liver shadow on the right side.
Abnormalities in situs can be situs inversus and situs ambiguous. Visceroatrial situs refers to the position of the atria in relation to stomach, spleen, liver and bronchi. In visceroatrial concordance, atrial situs corresponds to that of other viscera. If it is not so, it is called visceroatrial discordance. The left lung has two lobes and a relatively longer bronchus which is below the left pulmonary artery. This is known as hyparterial bronchus. Right lung has three lobes and a wider, shorter bronchus which is above the right pulmonary artery. Right bronchus is eparterial. Cardiac position is mentioned as levocardia, mesocardia and dextrocardia, depending on the location of cardiac mass within the thorax. Base apex axis is also considered in differentiating between levocardia and dextrocardia. Usually the base apex axis and the cardiac position based on the cardiac mass in the thorax are concordant.
The three main cardiac segments are the atria, ventricles and great vessels. Connections between these three segments are also evaluated sequentially. Identification of each segment is based on its morphological characteristics.
Atrial situs is defined by morphological features including the appendages. Venous connections or position in the body cannot be used for definition in segmental analysis as they may vary. Atrial situs solitus is morphological left atrium on the left side and morphological right atrium to the right. Reverse pattern is atrial situs inversus. In atrial situs ambiguous or atrial isomerism, both atria will be either morphological right atrium or left atrium. Atrial isomerism is associated with left-right symmetry of abdominal organs, known as heterotaxy syndrome [2]. Due to the need for identification of visceroatrial situs, echocardiography in children usually starts with the subcostal view unlike the parasternal long axis view in adults.
Venoatrial connection is assessed by identifying the position of vena cavae and pulmonary veins. Inferior vena cava is normally to the right of the abdominal aorta. This relation is reversed in situs inversus. In most cases inferior vena cava drains to the right atrium. All four pulmonary veins can be seen in a modified high parasternal view in children and is known as crab view. Common venous chamber and pulmonary veins in supracardiac and cardiac forms of total anomalous pulmonary venous connection can also be seen in a similar modified parasternal short axis view.
Ventricular situs is depending on the morphology of the ventricles. As the atrioventricular valves go with the ventricles, morphological right ventricle has the tricuspid valve and morphological left ventricle has the mitral valve. In abnormal situations, they are referred to as right atrioventricular (AV) valve and left AV valve. Usually, the distally placed valve is taken as the tricuspid valve. The tricuspid valve has an attachment to the ventricular septum while the mitral valve does not have an attachment to the septum. But the position of atrioventricular valves is not useful in the presence inlet type of ventricular septal defect where the AV valves are at the same level. Right ventricular trabeculation is more coarse than the left ventricular trabeculation. Right ventricle has an infundibulum which separates the tricuspid and pulmonary valves. As there is no conus on the left side, there is mitral aortic continuity. This is a fibrous continuity between the non coronary aortic cusp and the base of the anterior mitral leaflet [2].
Atrioventricular concordance is assessed next. When the morphological right atrium and left atrium connect to the corresponding morphological ventricles, it is known as atrioventricular concordance. The reverse pattern is known as atrioventricular discordance. Ventriculoarterial relationships are also mentioned in this pattern. In usual dextrotransposition of great arteries, there is atrioventricular concordance and ventriculoarterial discordance. In corrected transposition, there is both atrioventricular and ventriculoarterial discordance so that it is physiologically corrected. Right atrial blood reaches the pulmonary artery through the left ventricle. Left atrial blood reaches the aorta through the right ventricle.
In normally related great arteries (NRGA), aortic valve is to the right and posterior to the pulmonary valve. Echocardiographic description of the relation between aorta and pulmonary artery is a circle and sausage appearance with right ventricular outflow tract and pulmonary artery encircling the aortic cross section.

In dextrotransposition of great arteries, the great vessels are almost parallel and the arrangement is called two circles appearance.
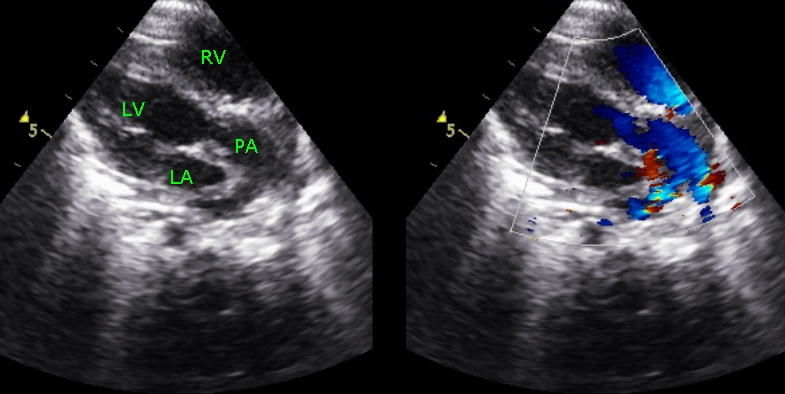
Aorta and pulmonary artery are identified by their arch and bifurcation respectively on tracing distally. Pulmonary artery arising from left ventricle is seen as the bifurcating vessel in the echocardiogram below:
This is a highly simplified version of the sequential segmental analysis in congenital heart disease. More detailed explanation with illustrations is available in the cited references.
References
- Lapierre C, Déry J, Guérin R, Viremouneix L, Dubois J, Garel L. Segmental approach to imaging of congenital heart disease. Radiographics. 2010 Mar;30(2):397-411.
- Shakya S, Rajashekar P, Gupta SK. Sequential Segmental Approach to Congenital Heart Disease. J Indian Acad Echocardiogr Cardiovasc Imaging 2020;4:244-52.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal