Supraventricular ectopics
Supraventricular ectopics
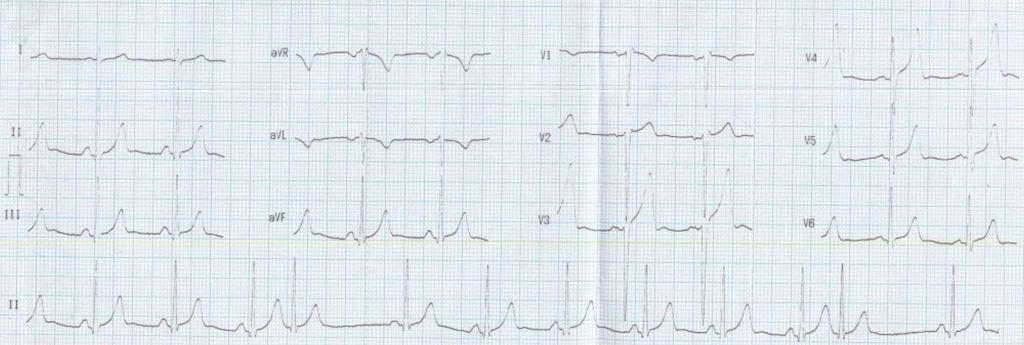
Supraventricular ectopics are premature beats originating above the ventricles. They have a narrow QRS complex and usually have a P wave with a different morphology from the sinus beats. If the supraventricular ectopic arises from the atrioventricular junction, the P wave may not be visible as it is hidden within the QRS complex as the activation of the atria and ventricles are nearly simultaneous. Sometimes a negative P wave after the QRS complex can be seen in low junctional rhythm.
Just as frequent ventricular ectopy can be the forerunner of ventricular tachycardia and ventricular fibrillation, frequent atrial ectopics can be the forerunner of atrial tachycardia and atrial fibrillation. In those with dual AV nodal physiology, an appropriately timed supraventricular ectopic will find the fast pathway refractory and conduct down the slow pathway. When it reaches the lower end, if the fast pathway has recovered, it conducts back, initiating a slow-fast type of reentrant AV nodal tachycardia (AVNRT).
Supraventricular ectopics can arise in multiple foci. If they occur at a rate above 100 per minute with three or more different P wave morphologies, it is known as multifocal atrial tachycardia (MAT). MAT is also called chaotic atrial rhythm. MAT can occur in those with chronic obstructive pulmonary disease.
Supraventricular ectopics can occur with stretching of atria due to overload. In acute myocardial infarction if frequent SVPCs are noted on the monitor, it is likely that there is left ventricular dysfunction producing left atrial overload due to elevated left ventricular end diastolic pressure. SVPC can also be a manifestation of hypertensive heart disease or other structural heart disease leading to left atrial enlargement and increased wall stress which could lead on to atrial fibrillation later [1].
Reference
- Tuan Le Nguyen, Liza Thomas. Supraventricular Ectopic Activity: When Excessive It Is Not All Benign! J Atr Fibrillation. 2010 Aug 23;3(2):307.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal