WPW syndrome ECG with disappearance of pre-excitation later
WPW syndrome ECG with disappearance of pre-excitation later
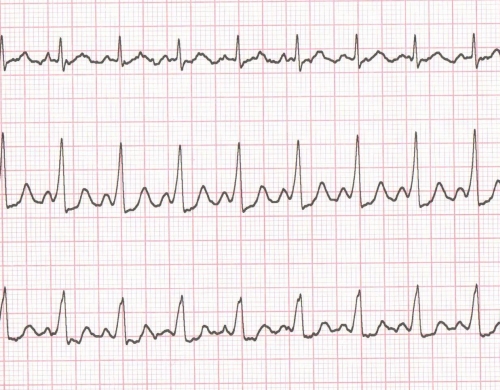
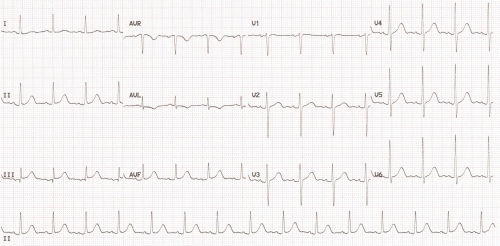
Features suggestive of WPW syndrome in this ECG are short PR interval and delta waves. In lead I delta wave is almost isoelectric and pre-excitation can be missed. Delta waves and QRS complexes are negative in aVR and aVL, while it is positive in all other leads.
Pathway localization: Left lateral pathway as there is a negative delta in aVL and V1-V6 positive.
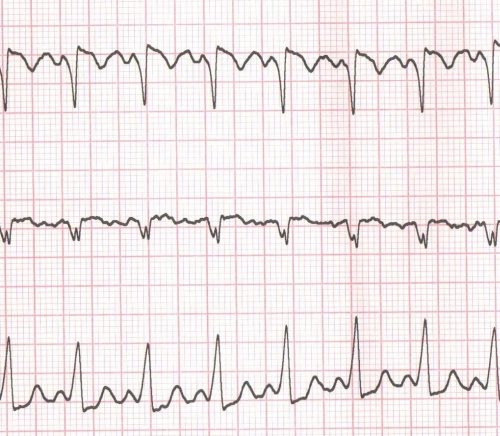
Repeat ECG after three days showing disappearance of pre-excitation
Repeat ECG after three days showing disappearance of pre-excitation. No pre-excitation is seen in this repeat ECG, meaning that there is no conduction through the accessory pathway. Initial deflection in Lead 1/aVL are positive, R/S in V1 is less than 1. That would mean the absence of two most sensitive indicators of anterograde conduction through left lateral pathway.
This can happen due to three possibilities: (1) Block at accessory pathway, (2) Interatrial conduction delay as suggested by the notched P wave in lead 1, or (3) Accelerated conduction through AV node; akin to the disappearance of accessory pathway conduction with stress test. The last one is not applicable here.
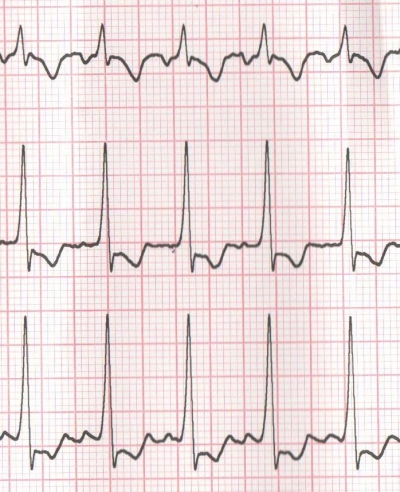
The initial two cannot be differentiated in surface ECG. Of course some soft pointers may give some clue: 1. If an atrial premature complex from left atrium results in pre-excitation, second factor is negated. 2. Notched P has been suggested as an evidence of interatrial conduction delay or delay at Bachman Bundle.
Left lateral pathways are well known to have no pre-excitation on surface ECG due to some of these reasons and may manifest with atrial pacing only. Then it is known as latent pre-excitation.
Spike and dome P wave is classically described with left upper pulmonary vein focus. It was earlier put as left atrial rhythm. But that pattern is seen only when the rhythm is from lateral left atrium with delayed right atrial activation.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal