Giant T wave inversion
Brief Review
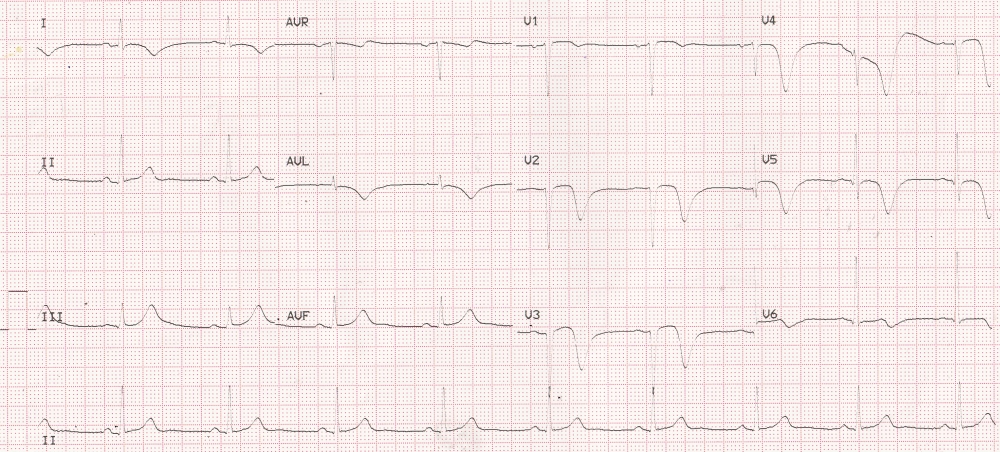
ECG showing deep T wave inversion in anterior wall myocardial infarction
Giant T wave inversion can be broad and deep or just deep T inversions. A depth of T wave of 10 mm or above is generally considered as deep T inversion [1]. Giant T wave inversions with depth of 35 mm have also been described in literature [2]. Deep T inversions without gross increase in width can occur in ischemia and hypertrophic cardiomyopathy. In a study involving 864 patients with hypertrophic cardiomyopathy, 15% had giant T wave inversion [3]. While giant T inversions occurred in about one third of patients with apical hypertrophic cardiomyopathy, it was seen in only 6.2% of those with asymmetric septal hypertrophy and one fourth of those with mixed pattern of hypertrophy. But there was no significant correlation between the apical myocardial thickness and the amplitude of T wave inversion.
In ischemia the width may sometimes be increased. Absence of left ventricular hypertrophy and symmetric nature of the T inversion (as in the ECG illustrated) has been suggested as indicators of myocardial ischemia in giant T wave inversion [4]. Deep and wide negative T waves are an important feature of post anoxic state and occurs typically after a Stokes-Adam attack. Presence of such broad and negative T waves in a case of complete heart block would indicate that the person had a recent episode of asystole. Since the QT interval is grossly prolonged in that situation, there is a high chance of polymorphic ventricular tachycardia (torsades des pointes). Giant wide T inversion can occur in intracranial bleeds like subarachnoid hemorrhage. Giant T wave inversion has been reported in pheochromocytoma, after electroconvulsive therapy [1] and Takotsubo cardiomyopathy [5]. Giant T wave inversion can also occur with cardiogenic, but non ischemic pulmonary edema, associated with prolongation of QT interval and resolving after resolution of symptoms [6].
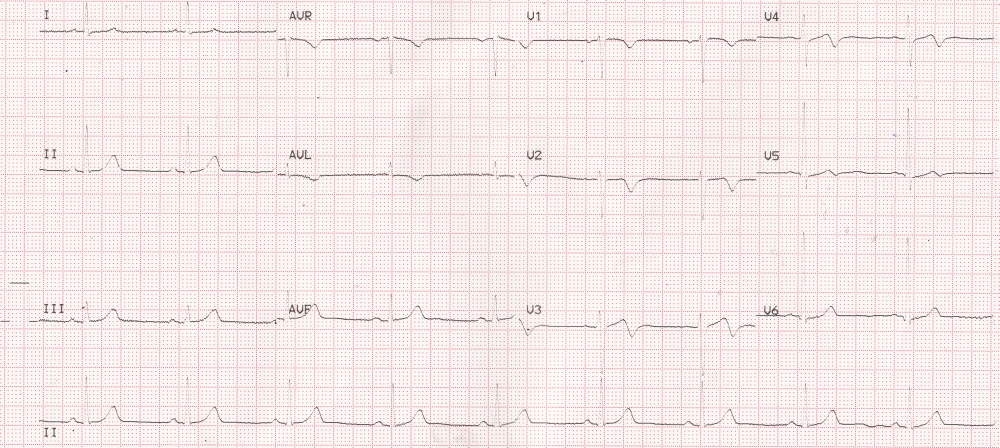
ECG showing reduction in the amplitude of T wave inversion in the same case
References
- Said SA, Bloo R, de Nooijer R, Slootweg A. Cardiac and non-cardiac causes of T-wave inversion in the precordial leads in adult subjects: A Dutch case series and review of the literature. World J Cardiol. 2015 Feb 26;7(2):86-100.
- Yue-Chun L, Lin JF. Rare giant T-wave inversions associated with myocardial stunning: report of 2 cases. Medicine (Baltimore). 2014 Jun;93(4):e39.
- Kim SH, Oh YS, Nam GB, Choi KJ, Kim DH, Song JM, Kang DH, Song JK, Kim YH. Morphological and Electrical Characteristics in Patient with Hypertrophic Cardiomyopathy: Quantitative Analysis of 864 Korean Cohort. Yonsei Med J. 2015 Nov;56(6):1515-21.
- Otrusinik R, Alpert MA, Hamm CR, Bikkina M, Porubicin M, Panayiotou H. Factors predicting coronary artery disease in patients with giant negative T waves. Am J Cardiol. 2000 Apr 1;85(7):873-5, A9.
- Yaguchi M, Yaguchi H, Takahashi N. A case of asymptomatic takotsubo cardiomyopathy with intraventricular thrombus associated with epileptic seizure. Brain Nerve. 2011 Aug;63(8):897-900.
- Littmann L. Large T wave inversion and QT prolongation associated with pulmonary edema: a report of nine cases. J Am Coll Cardiol. 1999 Oct;34(4):1106-10.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal