Palpation of precordium and adjacent areas
Palpation of precordium and adjacent areas
Palpation initially confirms the findings of inspection and further looks for new findings.
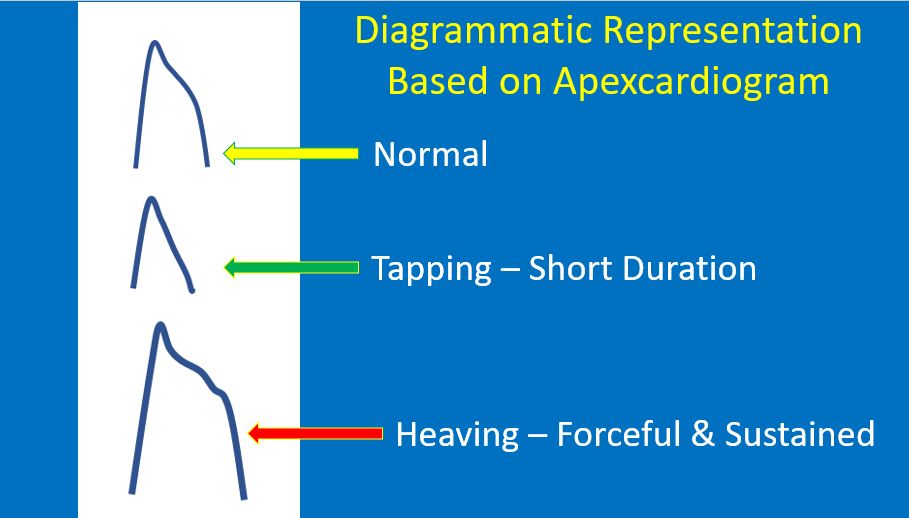
- Apex beat: Apex beat is defined as the lowest and outer most point of definite cardiac impulse. If apex beat is not felt on left side, immediately check on right side or else we might miss a dextrocardia. There some who even palpate both sides simultaneously for this reason. Apex beat is initially felt with the palm of the hand and then localized with the index finger. Sometimes it may be difficult to palpate in obese individuals and in those with emphysema. Palpation in held expiration and in the left lateral position may help in localization. Normal apex beat is felt in the 5th left intercostal space, typically about 1 cm medial to the midclavicular line. Tapping apex beat is the palpable counterpart of a loud first heart sound in mitral stenosis. A forceful apex beat is seen in regurgitant lesions like aortic and mitral regurgitation. It is also called a hyperdynamic apex. Heaving apex beat is both forceful and sustained, and is characteristic of left ventricular hypertrophy of severe aortic stenosis. Dyskinetic apex in left ventricular aneurysm is a see-saw pulsation with an additional out of phase bulge above the lowest impulse. Point of maximum impulse is sometimes checked when the apical impulse is diffuse and difficult to localize. Pulse – apex deficit is a term used in atrial fibrillation to note the difference between the pulse rate and the rate of apical impulses. Pulse deficit is usually more than 10 per minute in atrial fibrillation as all beats may not have a good pulse in the fast irregular rhythm. Double apical impulse and triple apical impulse may be felt in hypertrophic obstructive cardiomyopathy. In hypertrophic obstructive cardiomyopathy, one of the impulses may be diastolic, being the palpable component of a loud fourth heart sound due to forceful atrial contraction.
- Left parasternal heave: Left parasternal heave is felt with the ulnar aspect of the palm which is kept perpendicular to the precordium. It is a feature of right ventricular hypertrophy. Hyperdynamic left precordial pulsations which are not so forceful can be noted in atrial septal defect with large left to right shunt even without severe pulmonary hypertension and right ventricular hypertrophy.
- Pulsations in second left intercostal space: Pulsations in left intercostal space indication enlarged pulmonary artery, are better felt with the finger tips, after flexing the proximal interphalangeal joints at right angle.
- Right parasternal pulsations: Right parasternal pulsations may be noted if the aortic root is grossly dilated.
- Epigastric pulsations: Epigastric pulsations can be due to right ventricular hypertrophy, hepatic pulsations in severe tricuspid regurgitation and aortic pulsations. Right ventricular pulsations will be felt on the tip of finger kept below the xiphoid process. It becomes more prominent in inspiration. In emphysema, when the left parasternal heave is not palpable, this may be the only sign of right ventricular hypertrophy. Hepatic and aortic pulsations will be felt on the ventral aspect of the finger.
- Hepatic pulsations: Hepatic pulsations are better felt by bimanual palpation with one hand over the right hypochondrium and another over the back. Presystolic pulsations are noted in tricuspid stenosis and systolic pulsations in tricuspid regurgitation.
- Suzman sign is the visible or palpable collaterals in the upper back in coarctation of aorta. They are seen better on bending forward.
- Thrills: Thrills are the palpable counterparts of cardiac murmurs and are generally associated with very loud murmurs (grade IV and above). Thrills are better appreciated with the ulnar aspect of the palm of the hand. Location and timing of thrill depends on the cause. Thrills can be systolic, diastolic or continuous. They can be timed with respect to the carotid pulse, just like murmurs. Thrill of aortic stenosis can be felt in the second right intercostal space or the left parasternal region. In pulmonary stenosis, it is present in the second left intercostal space. Both these are systolic thrills. Thrill of small ventricular septal defect (maladie de Roger) is systolic and noted in the left parasternal region. Systolic thrill of mitral regurgitation is felt at the apex. Diastolic thrill of mitral stenosis is highly localized to the apex. Diastolic thrill may occur in aortic regurgitation in the left parasternal region. Continuous thrill in the first and second left intercostal space is noted in patent ductus arteriosus.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal