Patent foramen ovale vs small ASD
Patent foramen ovale vs small ASD
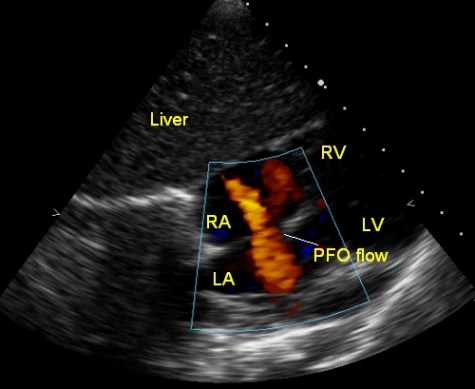
Patent foramen ovale vs small ASD: Echocardiogram from subcostal view showing the interatrial septum with a small defect and left to right flow across. Red colour encodes flow towards the transducer at the top and hence a flow from left atrium (LA) to right atrium (RA). Whether it has to be called a small atrial septal defect (ASD) or a patent foramen ovale (PFO) is the question. Conventionally PFO is a valvular opening which closes when the blood tries to flow from the left atrium to the right atrium. In certain phases of the cardiac cycle or during a Valsalva maneuver, right to left flow of blood can occur across the PFO. This is thought to be the mechanism of paradoxical embolism and stroke in case of PFO. Left to right shunt can occur across a stretched open PFO when the right or left atrium enlarges due to another pathological condition which elevates the left atrial pressure. In this case there was an associated ventricular septal defect (VSD). But the size of the defect and the magnitude of the shunt across the VSD was not sufficient enough to produce volume overloading of the left sided chambers.
If there is a spontaneous left to right shunt through out the cardiac cycle, the defect is better considered as a tiny atrial septal defect rather than a PFO. The reason is that PFO by definition, is a valvular opening which permits shunting only right to left. PFO shunts can be detected by saline contrast echocardiography in which agitated saline is injected into a peripheral vein. If the contrast appears in the left atrium within three cardiac cycles, it is suggestive of right to left shunt across the PFO. Trans esophageal echocardiography may be better for the demonstration of PFO because of higher resolution.
Transcranial Doppler studies will document these bubbles reaching the brain and hence the possibility of paradoxical embolism and stroke in case there is deep vein thrombosis. PFOs have also been associated with migraine like symptoms. Whether these are also related to paradoxical emboli has to be considered.
PFO closure has been recommended for the secondary prevention of stroke as well as for primary prevention of stroke in case of transient ischemic attacks. PFO closure device is similar to the ASD closure device, but differs in two aspects. The right atrial disc is larger, unlike the ASD device. The connecting piece between the two discs is of much lesser diameter compared to an ASD device. The technique of device delivery is similar to that of ASD device closure. Device closure is done under fluoroscopy in the cath lab with guidance of device position by trans esophageal echocardiography.
Management of patients with patent foramen ovale and cryptogenic stroke has been reviewed by Abdelghani M and colleagues [1]. They have reviewed multiples trials and meta-analyses of PFO device closure and given an algorithm.
Reference
-
Abdelghani M, El-Shedoudy SAO, Nassif M, Bouma BJ, de Winter RJ. Management of Patients with Patent Foramen Ovale and Cryptogenic Stroke: An Update. Cardiology. 2019;143(1):62-72.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
Add a Comment
You must be logged in to post a comment.
Thanks for clarifying the difference between a small ASD and a PFO.
Very nice and informative way of describing difference between pfo and asd thanks